Lesson 3 - Stereotypes, Labels, Sample Size, and Side Effects
| Site: | MoodleHUB.ca 🍁 |
| Course: | Abnormal Psychology 35 RVS |
| Book: | Lesson 3 - Stereotypes, Labels, Sample Size, and Side Effects |
| Printed by: | Guest user |
| Date: | Thursday, 30 October 2025, 1:14 AM |
Section/Lesson Objectives
The student will ...
• understand and describe the five major perspectives of psychologists
• differentiate between the six views of abnormality
• apply the definition of abnormal behaviour used in this course
• explain how abnormal behaviour was viewed and treated in the past
• state the contributions of various historical figures to our current understanding of mental illness and treatment
• understand the effects of stereotyping and labelling on mental health [This lesson]
• describe the consequences associated with a self-fulfilling prophecy [This lesson]
• learn about the side effects of medications as well as their effects on the brain [This lesson]
• differentiate between the five types of reliability and three types of validity
• understand and describe the North American classification system for mental disorders
• describe the importance of clinical interviews and testing
Introduction
As discussed in your first lesson, our biases affect how we interpret the world around us and how we approach the treatment of abnormal behaviour. Nowadays, many misconceptions and erroneous stereotypes continue to plague contemporary society. Psychologists and other academics once thought that only bigoted people employed stereotypes but, in reality, all of us use stereotypes to some degree, many of which are subconscious. Can you think of a stereotype that you might hold? Our expectations and stereotypes of the woman's role in society has certainly changed over the years. But do some stereotypes still exist today?
Stereotype
Originally referring to an old-fashioned printing technique, a stereotype was an impression taken from lead type (letters, numbers, and symbols) such that subsequent copies of documents could be made with no changes - essentially a fixed pattern. This technique was generalized into a metaphor for repeating a set of ideas with no changes. Today’s definition of a stereotype remains, in essence, as an oversimplified opinion or an uncritical judgement of some group of individuals who share certain characteristics or qualities.
Stereotyping is often used negatively and, according to Mahazarin Banaji (a psychology professor at Yale University), is “alive and well.” Banaji compiled research data that indicates that, while obvious bigotry may be declining slightly, stereotyping is still prevalent and presents a huge social problem.
To make sense of the world and to give order to our thoughts, we use categories to group people, places, and things. In fact, our ability to categorize and evaluate helps define humans as intelligent beings. Unfortunately, however, categorization has its drawbacks. We have been socialized by family, friends, media, and life experiences, for example, to categorize without sufficient information, to categorize from erroneous information, and to categorize based on atypical experiences. According to Banaji, when we use stereotypes, we observe the gender, age, skin colour, education, and wealth of a person, and our minds respond with messages such as hostile, stupid, slow, lazy, and/or weak. These qualities are not explicit upon looking at a person and/or his or her belongings. These are traits we have ascribed to individuals in the groups into which we have categorized them. Much of this categorization occurs subconsciously and is quite difficult to identify. In short, to confront stereotypes, some of which we do not even know we hold, is quite a challenge.
Take a moment to view the video below that ran as a commercial during the super bowl XLIX broadcast. What do you think of when you hear "...like a girl." added to a skill? This is a great example of a stereotype that many people hold which clearly has no merit.
Common Stereotypes
Mental illness is a topic that many people associate with stereotypes. Alot of this due to the fact that few people are educated on this topic, unless it has affected them personally. Negative perceptions of mental illness colour the support and advice people get from their friends, family and even their physicians and can create a reluctance to seek help. One in five Canadians are affected by mental illness and many of them do not seek help because they are afraid to talk about it. Refer to the table below that displays some of these common stereotypes.
Table: Common Stereotypes
| Popular Myths and/or Erroneous Stereotypes |
Fact |
| 1. Abnormal behaviour is consistently bizarre. | The behaviour of most mentally ill individuals is often impossible to differentiate from that of“normal” individuals. |
| 2. Mentally ill individuals are unpredictable and dangerous. | Mentally ill individuals are no more dangerous than the general population. There may be more publicity and media coverage, however, with crimes committed and behaviours exhibited by the mentally ill. |
| 3. Mental disorders are due to fundamental personal deficits and, therefore, are shameful. | Everyone shares the potential for mental illness and abnormal behaviour. |
| 4. Individuals never fully recover from mental illness and should be approached with caution. | A full recovery is possible as is integration into the general population. |
| 5. The mentally ill are weak and could recover from their illness if only they put effort into changing. | Mental illness can happen to anyone; it is not related to strength or weakness of character. |
| 6. Only those of lower intelligence become mentally ill. | Intelligence has nothing to do with mental illness; everyone shares the potential for abnormal behaviour regardless of IQ. |
Let's Change Negative Stereotypes!
Work is being done to educate people about mental illness and to change the stigma surrounding the topic. You may have seen advertisements similar to those below, designed to make people think about their views. As a society, we can be more accepting of physical illness and offer those that are suffering encouragement and support, however, we are afraid to address the topic of mental illness and turn our heads the other way.
Advertisements from the Canadian Psychiatric Research Foundation

|
What is Stigma? In the context of mental health, stigma is the use of negative labels to identify a person living with mental illness. It is about disrespect and keeps mental illness in the closet. Stigma is a barrier and discourages individuals and their families from getting the help they need. It closes minds and fuels discrimination. Many say that living with the stigma is worse than living with the illness itself. (Canadian Mental Health Association) |
Video: Stigma
Watch the video below where Stella relays her experience with bipolar disorder and the stigmas that she has had to face and overcome.
 After you have watched the video, you will need to make a journal entry.
After you have watched the video, you will need to make a journal entry.
Bell Canada's launched a "Let's Talk" campaign, led by Olympian Clara Hughes. The goal of this campaign is to raise awareness and to talk openly about mental illness. Watch the video below to learn about Clara's big ride which she used to start the conversation about mental illness. As a society, we need to change the stigma associated with mental health.
Self-fulfilling Prophecy
Related to stereotypes is the concept of labeling. Labeling relates to the image we have of ourselves and others, both positive and negative, based upon the message others communicate to us. If we employ a specific label, for example, then we expect specific behaviour from people who have that label. The behaviour expected from various labels, whether accurate or not, can become real or true because of having been predicted or expected. This is called a self-fulfilling prophecy.
 A student, Kayla, did poorly on an English assignment. Her teacher may have told her that she is weak in grammar. She then begins to think that she is “bad” at English overall and, over time, may expect that she will do poorly on any English assignment. Because of this belief, she puts little effort into learning grammar. Kayla believes that any effort would be wasted because she is not good at English – so why bother trying? What Kayla does not realize is that her lack of success in English may be due to insufficient effort. Her perception of her lack of ability, however, has made it impossible to realize that something could help her. Because of this, she has fulfilled the prophecy that she is poor at English. How would this self-fulfilling prophecy work differently in this case, if Kayla's teacher told her that she was an excellent English student?
A student, Kayla, did poorly on an English assignment. Her teacher may have told her that she is weak in grammar. She then begins to think that she is “bad” at English overall and, over time, may expect that she will do poorly on any English assignment. Because of this belief, she puts little effort into learning grammar. Kayla believes that any effort would be wasted because she is not good at English – so why bother trying? What Kayla does not realize is that her lack of success in English may be due to insufficient effort. Her perception of her lack of ability, however, has made it impossible to realize that something could help her. Because of this, she has fulfilled the prophecy that she is poor at English. How would this self-fulfilling prophecy work differently in this case, if Kayla's teacher told her that she was an excellent English student?
Please watch the video below on the self fulfilling prophecy. An example is provided at the end of the video. Their are many aspects to our lives that the self-fulfilling prophecy can be applied to.

Unfortunately, many people are given messages that may be based on inaccurate or incomplete information. According to some sociologists, many individuals give us damaging messages that result in the development of our own self-fulfilling prophecies.
Examples of people who give such messages include parents, teachers, judges, bankers, and employers. If a bank executive, for example, believes you are not likely to succeed, then, you will not get a loan, and you will not be given the chance to prove yourself successful. Unfortunately, a positive feedback cycle often occurs after an individual has been labelled negatively. With a self-fulfilling prophecy (brought on by an inaccurate label), the belief that something is true about individuals or groups can cause them to act in ways to actualize the prophecy. The fulfillment of the self-fulfilling prophecy can often result in a stigma.
Research Samples
Another problem with labelling involves sampling. Researchers in the late twentieth century designed experiments that focused on one subset of individuals and then assumed the results applied to everyone. For example, much research was done using Caucasian adult males. The results were then “carried over” or ascribed to women (who are not men), children (who are not adults), and men who were not Caucasian. Researchers discovered that the results could not simply be transferred to other demographic groups. How women, children, and other races respond to drugs, therapies, and other treatment methodologies is often different from how a Caucasian adult male responds. With psychological research, any study that uses only white males must ascribe any outcome only to white males, not to children, women, or other races. In some cases, a medication that is effective for an adult is ineffective for a child; in some cases it even has the opposite effect. In other cases, sometimes a smaller dose or larger dose of a medication has the same effect on a child that a standard adult dose has on an adult. Fortunately, current researchers take into account the fact that there are marked differences between adults, children, and adolescents in addition to men, women, and people of different races.
 Not long ago scientists realized they lacked the necessary tools to properly diagnose children. Advances in this area are being made, but the long-term consequences of medication-based treatment have not been sufficiently documented. Many child psychologists note that non-pharmaceutical treatments can drastically reduce or even eliminate the need for medication in some children. Cognitive behavioural therapy, for example, helps children learn to manage their thoughts and control their behaviour. Some individuals, however, may need medications for the more debilitating symptoms despite side effects such as weight changes, jitteriness, or a dulled/flattened personality.
Not long ago scientists realized they lacked the necessary tools to properly diagnose children. Advances in this area are being made, but the long-term consequences of medication-based treatment have not been sufficiently documented. Many child psychologists note that non-pharmaceutical treatments can drastically reduce or even eliminate the need for medication in some children. Cognitive behavioural therapy, for example, helps children learn to manage their thoughts and control their behaviour. Some individuals, however, may need medications for the more debilitating symptoms despite side effects such as weight changes, jitteriness, or a dulled/flattened personality.
In studies published in the Archives of Clinical Neuropsychology and Attention Deficit Hyperactivity Disorder, kids with ADHD who exercised performed better on tests of attention, and had less impulsivity, even if they weren't taking stimulant medicines. Many kids with ADHD also struggle socially and with their behavior. Playing a sport can have the added benefits of improving both of these areas. (WebMD)
(http://www.webmd.com/add-adhd/childhood-adhd/exercise-for-children-with-adhd_?page=2)
The Brain
 Time Magazine (Canada, 2004) featured an article that exemplified the advantages and disadvantages of pharmaceutical-based treatment for children with abnormal behaviours. One of the individuals interviewed in the article, Jessi, speaks of the differences in her personality when she is taking her medication and when she is not taking her medication. This type of side effect, a marked difference in personality, is called emotional liability. Her story begins with a diagnosis of attention deficit hyperactive disorder (ADHD) in kindergarten. Being sent to the “time-out-chair” many times a day was the result of her inability to foresee the consequences of her actions. The first drug she tried took away her appetite completely; eventually, the doctors had to switch medications. While it is now working well, to find the proper dosage with the second drug took a long time . With this medication, Jessi is able to concentrate in school, but without it, she cannot focus on school work. While taking her medication, she is very shy and does not say much or participate in conversations. When off her medication, she is outgoing, spontaneous, and talkative. Having this emotional liability as a side effect sometimes depresses Jessi, but the alternative, the inability to focus, is worse.
Time Magazine (Canada, 2004) featured an article that exemplified the advantages and disadvantages of pharmaceutical-based treatment for children with abnormal behaviours. One of the individuals interviewed in the article, Jessi, speaks of the differences in her personality when she is taking her medication and when she is not taking her medication. This type of side effect, a marked difference in personality, is called emotional liability. Her story begins with a diagnosis of attention deficit hyperactive disorder (ADHD) in kindergarten. Being sent to the “time-out-chair” many times a day was the result of her inability to foresee the consequences of her actions. The first drug she tried took away her appetite completely; eventually, the doctors had to switch medications. While it is now working well, to find the proper dosage with the second drug took a long time . With this medication, Jessi is able to concentrate in school, but without it, she cannot focus on school work. While taking her medication, she is very shy and does not say much or participate in conversations. When off her medication, she is outgoing, spontaneous, and talkative. Having this emotional liability as a side effect sometimes depresses Jessi, but the alternative, the inability to focus, is worse.
The brain is the most complex organ in the human body. The structural and chemical composition of this organ is astounding. Formed and molded from interactions among our genes, life experiences, and environment, the brain receives, co-ordinates, and distributes information to orchestrate how we think, feel, learn, and behave. To perform these functions, the brain must effectively communicate with all its cells. Failure to do so may cause or contribute to brain dysfunction and mental illness.
Watch the video below on the teenage brain.
Please refer to the diagrams of the brain below, which shows the areas of the brain believed to be responsible for various afflictions. The table below explains the role that each part of the brain plays.
| Parts and Functions of the Brain | |
| Frontal Lobe | This part of the brain organizes, plans, and controls movement. Problems in this area may be linked to depression, ADHD, and obsessive-compulsive disorder (OCD). |
| Basal Ganglia | Within the limbic system, the basal ganglia control anxiety levels and co-ordinate motor behaviour. Difficulties in this area may be linked to panic, anxiety, OCD, depression, and bi-polarity. Also part of the limbic system is the putamen area. This area is linked to ADHD. |
| Hippocampus | This area is essential to the formation of memories and higher learning. Problems in this area may be linked to depression, anxiety, panic, and bi-polarity. |
| Amygdala | (Not labelled) This structure is the focal area for fear and emotion. Difficulties with this area may be linked to depression, anxiety, panic, and post-traumatic stress. |
| Prefrontal Cortex | (Not labelled) Responsible for the regulation of attention span and impulse control, this area is also important in problem solving, critical thinking, and the ability to empathize. Damage to this area may be linked to ADHD, OCD, anxiety, and bi-polarity. |
| Thalamus | This area can be considered the “dispatch station” for incoming sensory information. If the thalamus is not functioning properly, OCD symptoms may arise. |
| Cingulate Gyrus | (Not labelled) Cognitive flexibility, adaptability, and co-operation are some of the tasks for which this area is responsible. OCD is linked to damage in the cingulate gyrus. |
The Teenage Brain
Let's get a little bit more personal now and learn about how the teenage brain functions and changes that occur during the teenage years.
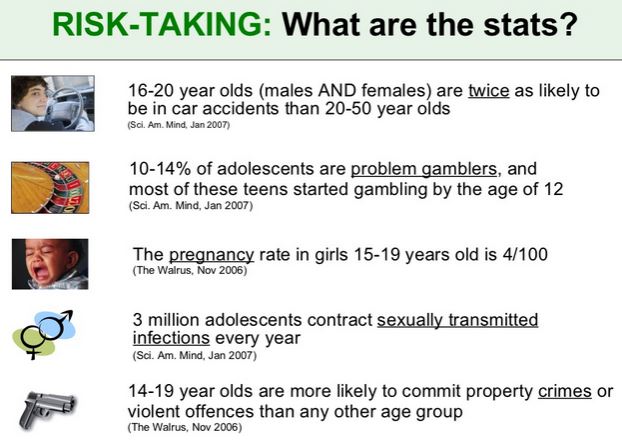
Adolescence is a time of growth and maturation in the brain. It is also a time when new behaviours begin to emerge; some of which become a great frustration and worry to parents. Changes that present themselves result from a change in motivation, attention and risk taking. Many cognitive abilities including the control of attention are controlled by the pre-frontal cortex. This part of the brain undergoes massive changes during adolescence and is one of the last areas of the brain to mature completely. Teenagers are known for reckless, risk taking and impulsive behaviour. While some of this risk taking behaviour is considered normal and adaptive, it also puts the adolescence at a great risk for personal injury. The dangerous scenario occurs when teens act spontaneously and do not consider the possible consequences of their actions.
|
Case Study Tragedy struck at Canada Olympic Park in Calgary a couple of years ago when eight teens climbed a fence and attempted to slide down the bobsled track on a toboggan. The toboggan slammed into a gate half way down the track killing two of the teens and sending several others to hospital with serious injuries. This is an example of an activity that sounded like fun where the teens did not fully comprehend and consider the consequences of their actions. Eg. How fast will we go? How will we stop at the bottom? What if someone gets hurt? What if we get caught? Could I get badly injured or die? Please read the article below on what the experts say are some of the reasons for teens participating in risk taking behaviour.
|
teenmentalhealth.org
Please watch the video below on the teenage brain which provides some interesting information about the growth and development of the teenage brain. The teenage brain is driven by the dopamine response. Dopamine is a neurotransmitter that plays a role in reward-motivated behaviour. Most types of reward increase the level of dopamine in the brain. In this video you will see how the development of the teenage brain in search of the dopamine response, can influence behaviour. When the outcome of a behaviour is good, the dopamine goes up and when the outcome is bad, the dopamine goes down. Because we like the dopamine rush we get from an activity, the brain remembers, and we do it again.

Video: Insight into the Teenage Brain, TED Talks (Length of video: 9:42 minutes). Note: See questions below that you will be asked to respond to in a journal entry after you have watched the video.
 |
 After watching the video "Insight into the Teenage Brain", you are required to make a journal entry.
After watching the video "Insight into the Teenage Brain", you are required to make a journal entry.
1. At what age does the brain develop until?
2. Does the brain develop from front to back OR back to front?
3. What is the role played by the prefrontal cortex?
4. What is the role played by the striatum?
5. How does the dopamine response influence behaviour?
6. Based on the research that was presented in this video using brain scans, what did you learn about how the sensitivity of the brain changes from childhood to teenager and then to adulthood? (3 marks)
7. When does the prefrontal cortex start to play a more active role in regulating behaviour?
8. What were the three "Take-Home" points noted? (3 marks)
9. Explain why the sensitivity of the teenage brain to rewards and emotions might lead teens to make poor choices. Provide an example.
b) Explain how this sensitivity could have a positive impact? Provide an example.
Total Marks = 14.
Approved Psychiatric Medications for Children in Canada
Approved Psychiatric Medications for Children in Canada
Note the side effects of each drug and how the drug works. Be aware that not every individual experiences the side effects associated with each medication.
| Name of Drug | How it Works | Side Effects | Target Age |
| Concerta | To reduce hyperactivity and inattention, this drug keeps neurons immersed in norepinephrine and dopamine. | Stomach pain, headache, sleeplessness, and, in rare cases, overstimulation | Approved for children aged 6 to 12 with ADHD |
| Ritalin | The active agent, methylphenidate, stimulates the brain to filter and prioritize incoming information. | Insomnia, nervousness, headache, decrease in appetite, and irritability | Approved for children with ADHD, 6 years and older |
| Lithium | This drug stabilizes episodes of elated and intensely joyous moods associated with mania. | Loss of appetite, nausea, and hand tremors | Cautiously prescribed pediatrically for bipolar disorder and as an agent for suicide prevention |
| Prozac | This antidepressent is aimed at regulating serotonin levels. | Weight loss, anxiety, insomnia, mania, and nervousness | Cautiously prescribed for children |
| Depakote | This anti-seizure medication is also used for treating the grandiose and hyper-agitated state of mania. | Nausea, headache, drowsiness, and white blood cell abnormalities | Cautiously used to treat childhood bipolar mania and seizures |
| Zyprexa | This mood stabilizer is designed to balance levels of serotonin and dopamine in the brain. | Dry mouth, seizures, weight gain, and drowsiness | Cautiously prescribed pediatrically for bipolar disorder, psychotic depression, and schizophrenia |
 Regarding drug therapy, many experts believe that medications are most effective when combined with counselling. For children with minor symptoms (for example, those who are sombre but not depressed, those who are fidgety but not hyperactive, those who demonstrate repetitive behaviours but are not obsessive-compulsive), the advantages and disadvantages of using drugs are not always obvious.
Regarding drug therapy, many experts believe that medications are most effective when combined with counselling. For children with minor symptoms (for example, those who are sombre but not depressed, those who are fidgety but not hyperactive, those who demonstrate repetitive behaviours but are not obsessive-compulsive), the advantages and disadvantages of using drugs are not always obvious.
Health care professionals must be careful with assessments of such children. Using medication to control or regulate “normal” variations in behaviour may be unnecessary, inappropriate, and/or unethical.
Lesson Review
Lesson 3 draws to a close. Were you overwhelmed by the amount of material and the number of different ideas presented? Do not dismay! You will likely find future lessons less hectic. If you have managed to understand the main ideas in the lesson notes and are ready to tackle some assignments, you have done well!
|
To summarize: • understand and describe • understand how the brain works, which area of the brain are believed to be responsible for various afflictions • know the psychiatric medications for children, the target age, how they work and what are the side effects |
Assignment
Journal Entry 1: Stigma
Complete a journal entry on stigma after watching the video provided in the lesson.
Journal Entry 2: Surviving the Teenage Brain
Complete the journal entry on the teenage brain after watching the video from The Nature of Things, "Surviving the Teenage Brain."