Lesson 4 - Assessment and the DSM-V
| Site: | MoodleHUB.ca 🍁 |
| Course: | Abnormal Psychology 35 RVS |
| Book: | Lesson 4 - Assessment and the DSM-V |
| Printed by: | Guest user |
| Date: | Thursday, 30 October 2025, 1:14 AM |
Section/Lesson Objectives
The student will...
• understand and describe the five major perspectives of psychologists
• differentiate between the six views of abnormality
• apply the definition of abnormal behaviour used in this course
• explain how abnormal behaviour was viewed and treated in the past
• state the contributions of various historical figures to our current understanding of mental illness and treatment
• understand the effects of stereotyping and labelling on mental health
• describe the consequences associated with a self-fulfilling prophecy
• learn about the side effects of medications as well as their effects on the brain
• differentiate between the five types of reliability and three types of validity [This lesson]
• understand and describe the North American classification system for mental disorders [This lesson]
• describe the importance of clinical interviews and testing [This lesson]
Introduction
 Before psychologists can begin treating a patient, they must determine, to the best of their ability, what exactly is bothering the patient. This is called assessment - the collecting of information about the patient and identifying causal factors in the person’s diagnosis. This information may include data regarding the person’s current symptoms, major life events, cognitive functioning, specific physical conditions, drug and alcohol abuse, and family history of illness.
Before psychologists can begin treating a patient, they must determine, to the best of their ability, what exactly is bothering the patient. This is called assessment - the collecting of information about the patient and identifying causal factors in the person’s diagnosis. This information may include data regarding the person’s current symptoms, major life events, cognitive functioning, specific physical conditions, drug and alcohol abuse, and family history of illness.
Collecting information in these areas helps psychologists make diagnosis and informed decisions regarding treatment options. Collecting information is not always easy for psychologists. In some cases time to collect the information is limited, the presenting problems may be extremely complex, and the medical and social history may be unknown. A psychologist must also take into account the patient’s capacity and willingness to participate in treatment. Will the patient have social support? Can he or she afford the treatment?
Reliability and Validity
The importance of the initial assessment is great. The initial assessment provides a baseline for later comparison and makes possible checking the effectiveness of the ongoing treatment to see if adjustments are necessary. For this reason, assessment must be reliable. With reference to psychological testing, reliability relates to the degree to which a measurement is consistent. Reliability can be divided into three categories: test-retest, internal, and inter-rater. The first category, test-retest reliability, requires that the psychologist obtain similar results with the same patient at two different points in time. With internal reliability, different parts of a test must produce similar results. In the last category, inter-rater reliability, two or more psychologists (or “raters”) must come to similar conclusions about the patient’s diagnosis.
Assessment must also be valid. Validity refers to the degree to which a technique or test measures what it is designed to measure. Validity can be divided into five categories. Face validity refers to a test or technique appearing to measure what it should measure. With content validity, the test or technique used actually measures the content or areas that are most important. The test or technique used may not measure everything, but it does not have to as long as it measures the major areas of concern. The third category, concurrent validity, requires that similar tests yield the same results. For example, two different I.Q. tests should yield similar results for the same individual. As the name suggests, predictive validity refers to how accurately behaviour can be predicted. For example, different patients with the same diagnosis are predicted to respond the same way to the same treatment. The last category of validity, construct validity, requires that a test measure what it is designed to measure. For example, if a test is designed to measure musical ability, actually measures verbal reasoning, it would not be considered a valid test.
Clinical Interviews
 Assuming that physical disease or illness has been ruled out, the first thing that many psychologists do with respect to assessment is a clinical interview. Clinical interviews examine current behaviours -- what people are doing in their daily lives, what their attitudes are concerning themselves and others, and what sort of problems they describe regarding themselves and their lives. Psychologists must be aware, however, that personal biases may affect how they perceive a particular patient. Using guidelines, structure, and a standardized set of questions may help reduce potential bias.
Assuming that physical disease or illness has been ruled out, the first thing that many psychologists do with respect to assessment is a clinical interview. Clinical interviews examine current behaviours -- what people are doing in their daily lives, what their attitudes are concerning themselves and others, and what sort of problems they describe regarding themselves and their lives. Psychologists must be aware, however, that personal biases may affect how they perceive a particular patient. Using guidelines, structure, and a standardized set of questions may help reduce potential bias.
Some clinicians use mental status exams to guide their assessments. With this type of exam, a psychologist can better determine the mental health of individuals. This test may also assist the psychologist in forming an hypothesis about a person’s pathologies. Perhaps the first area that an interviewer observes is appearance and behaviour. Are patients well-groomed with clean clothes? Have they bathed in the last six days? How is their posture? What is their behaviour like – are they tense, upset, or calm? The next area of interest may be thought processes. Do they have continuity of thought? Do they speak slowly or rapidly? What do they speak about?
The patients’ mood and affect also are areas of concern to the psychologist. What is the overall mood from day to day? Is the affect of a person congruent with the content of what he or she is saying? For example, is the person recounting a tragic event while smiling? Of equal importance, is the person recalling an emotionally charged event without emotion of any sort – is he or she just sitting there? Psychologists also like to understand the intellectual functioning of their patients. Do they use multi-syllable words? Do they use metaphors, similes, and abstractions? Can they clearly explain memories? Finally, are patients aware of their situation? Are they aware of their surroundings? Do they know their names, the date, or where they live?
Observation and Assessment
Psychologists assess the behaviour of others either by direct observation or by listening to an accounting of previous behaviour. They are careful to make note of antecedents (previous circumstances) that may relate to the problem. They look for factors, triggers, or events that were there when the problem behaviour started. They look at where and when the problem occurs and with whom the problem occurs. For example, a child may have behavioural problems at home but not at school. Psychologists may need to observe the child in both locations over a period of time. Psychologists would note the differences in the child’s behaviour in each situation, as well as how the child is being treated by the people in each environment. They may even wonder how the child feels in each situation – something not necessarily observed easily!
Testing
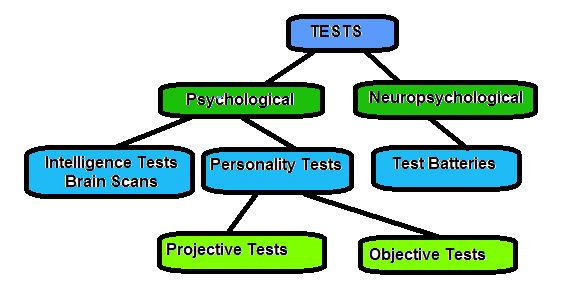
Behavioural observations and interviews are direct attempts to determine a patient’s attitudes and problems. Tests, on the other hand, are a more indirect (and often more objective) method of assessing characteristics. There are two types of tests most commonly used by psychologists: psychological tests and neuropsychological tests. They are used to determine cognitive, emotional, or behavioural responses that might be associated with specific disorders. The first category, psychological, includes tests of intelligence and personality. Intelligence tests are in many different forms and measure many aspects of cognitive functioning. Most intelligence tests take a long time to administer, score, and interpret. In many cases, knowing a patient’s intelligence quotient (IQ) is not required for successful treatment; thus, the financial cost of administering the test is simply too great and the test is not administered.
Ink Blot Examples

 Personality tests can be grouped
Personality tests can be grouped  into projective and objective tests. Projective tests are unstructured. They are based on the theory that people are not always aware of their feelings and, if given the opportunity, will project their feelings onto other objects, situations, or people. One famous projective test is the Rorschach Inkblot Test designed in 1911 by Swiss psychiatrist Hermann Rorschach. Originally designed to study perception, the Inkblot test was later used to study psychological disorders. Unfortunately, this test has limited reliability and validity. For example, if two psychologists were asked to make a conclusion based on the results of an Inkblot test for the same patient, they may not agree and they would not come to the same conclusions.
into projective and objective tests. Projective tests are unstructured. They are based on the theory that people are not always aware of their feelings and, if given the opportunity, will project their feelings onto other objects, situations, or people. One famous projective test is the Rorschach Inkblot Test designed in 1911 by Swiss psychiatrist Hermann Rorschach. Originally designed to study perception, the Inkblot test was later used to study psychological disorders. Unfortunately, this test has limited reliability and validity. For example, if two psychologists were asked to make a conclusion based on the results of an Inkblot test for the same patient, they may not agree and they would not come to the same conclusions.
The Thematic Apperception Test (TAT) is similar to the Rorschach Inkblot test. This test was developed in 1935 by Morgan and Murray of the Harvard Psychological Clinic. During testing, patients are shown cards with simple pictures on them. They are then asked to make up stories. The TAT generally requires much time to administer and has, like many other tests of this type, low reliability, questionable validity, and standardization problems. In short, these types of tests cannot predict psychopathology.
Objective tests, unlike projective tests, are structured. They typically use questionnaires, inventories, or rating scales to help assess personality. One well-known test in this category is the Minnesota Multiphasic Personality Inventory (MMPI). Developed in 1943 by Hathaway and McKinley, the MMPI continues to be widely used in many countries. This test asks over 500 questions and uses 10 clinical scales, 4 special scales, and 4 validity scales. The validity scales are aimed at identifying faking – the difference between people who do have psychological illness and the ones who pretend to have psychological illness. The Lie scale, for example, measures the tendency of people to claim excessive virtue -- the tendency of wanting to present an overall favourable image. The Infrequency scale measures a tendency to claim psychological problems falsely. All tests have shortcomings, however, and the original MMPI was criticized for its sexist wording, cultural insensitivity, and poor sample selection for its initial standardization. As a response to the criticism, the MMPI-2 was created in the 1980s. The test now has updated language and improved reliability and validity.
Neuropsychological Tests
In addition to a general medical examination, specialized neurological tests may be performed on patients. This type of testing is done because some mental disorders are directly linked to brain pathology. Clinicians use both neurological test batteries (a battery is a grouping of specific tests) and brain scans to assist in describing the brain-behaviour relationship. Two of the main neuropsychological batteries are the Luria-Nebraska and the Halstead-Reitan. These tests are administered in an attempt to locate and identify brain damage. Despite the occurrence of false-positives (test results that indicate brain damage where there is none) and false-negatives (test results that indicate no brain damage where there is some), the Halstead-Reitan is a reasonably reliable tool.
As noted previously, neuropsychological tests are used in conjunction with brain imaging tests to help determine areas of brain damage. These imaging tests include computerized axial tomography (known as CAT scans or CT scans), magnetic resonance imaging (MRI scans), electroencephalograms (EEGs), and positron emission tomography (PET scans). CT scans use x-rays; a narrow x-ray beam is passed through a person’s head and the amount of radiation absorbed is measured. The images produced show the brain in three different dimensions. From these images, structural abnormalities (injury and/or tumors) can be identified.
EEGs are used to assess general brain-wave patterns. They are obtained by placing electrodes on the scalp and recording brain-wave impulses. The pattern of these impulses can indirectly reveal abnormal brain-wave patterns and brain abnormalities such as brain lesions. PET scans, on the other hand, measure metabolic activity. In this scan, a harmless radioactive isotope is passed into the brain. This allows the clinician to see which areas of the brain are the most active. For example, they help pinpoint sites responsible for epileptic seizures. Using very large magnets, MRIs provide detailed pictures of the brain at any angle. An MRI can examine structure and function simultaneously. People with any metal in their bodies, however, cannot be scanned using this equipment because the metal would be pulled out of their body by the magnet! Refer to the chart below to see summary of tests.
Chart of Tests
Diagnosis and the DSM (DSM-V)
Diagnosis (the identification of a disease from a collection of signs and symptoms) is dependent on classification. If a friend told you that a yellow rose had bloomed in his garden the other day, you would have an accurate idea of what that rose looked like - not because you actually saw the rose, but from your knowledge of the categorization of roses. With abnormal behaviour, classification involves the description of various types or groups of maladaptive behaviour. Classification is based on generalizations formed from observations. Even with the best observations, generalizations include biases and inferences and may exclude cultural variations. To illustrate, a Native American hears the voice of a recently deceased loved one calling from the grave. He or she may view this experience as normal, but a person of European descent may label this an auditory hallucination.
Gender bias may also be prevalent in the classification done by clinicians. In one study where men and women displayed the same behaviour, clinicians were more likely to diagnose the women with histrionic personality disorder and the men with anti-social personality disorder (Ford and Widiger, 1989). Psychology is not an exact science!
Diagnosis in North America is guided by the Diagnostic and Statistical  Manual (DSM). The DSM has been revised many times. The original DSM, inspired by Kraepelin of the late nineteenth century, was published in 1952 by the American Psychiatric Association (APA). With each revision of this classification manual, changes are made that impact the way disorders are classified and diagnosed. The manual covers all mental health disorders for both children and adults. It also lists known causes of these disorders, statistics in terms of gender, age at onset, and prognosis as well as some research concerning the optimal treatment approaches. The latest version of this manual DSM-V was released in 2013. Any classification system has benefits and limitations, however, and health care practitioners must keep this in mind.
Manual (DSM). The DSM has been revised many times. The original DSM, inspired by Kraepelin of the late nineteenth century, was published in 1952 by the American Psychiatric Association (APA). With each revision of this classification manual, changes are made that impact the way disorders are classified and diagnosed. The manual covers all mental health disorders for both children and adults. It also lists known causes of these disorders, statistics in terms of gender, age at onset, and prognosis as well as some research concerning the optimal treatment approaches. The latest version of this manual DSM-V was released in 2013. Any classification system has benefits and limitations, however, and health care practitioners must keep this in mind.
 One of the limitations of the DSM classification system is the simplification of the definition of each type of illness. Mental illness is rarely simple and whether a person has an illness will establish whether (and how) he or she is treated. This is particularly important because with some diagnoses medication is prescribed, and the classification will determine which class of drugs will be used to treat the illness. For example, antidepressants are often used for depression, and tranquilizers are used to treat schizophrenia. An incorrect diagnosis in this example means that the incorrect medication is prescribed, which could do more harm than good. Also, diagnosis essentially labels a person. Labelling, as noted previously, can be extremely damaging. Labels describe the behaviour of a person – but not the actual “person” in his or her entirety. Note the following example, recounted by Carson, Butcher, and Coleman (1988), of how damaging a label can be.
One of the limitations of the DSM classification system is the simplification of the definition of each type of illness. Mental illness is rarely simple and whether a person has an illness will establish whether (and how) he or she is treated. This is particularly important because with some diagnoses medication is prescribed, and the classification will determine which class of drugs will be used to treat the illness. For example, antidepressants are often used for depression, and tranquilizers are used to treat schizophrenia. An incorrect diagnosis in this example means that the incorrect medication is prescribed, which could do more harm than good. Also, diagnosis essentially labels a person. Labelling, as noted previously, can be extremely damaging. Labels describe the behaviour of a person – but not the actual “person” in his or her entirety. Note the following example, recounted by Carson, Butcher, and Coleman (1988), of how damaging a label can be.
 Gladys Burr was involuntarily committed by her mother (apparently because of some personality problems) in 1936 at the age of 29. She was diagnosed as psychotic and later declared to be mentally retarded. Though a number of IQ tests administered from 1946 to 1961 showed her to be of normal intelligence, and though a number of doctors stated that she was of normal intelligence and should be released, she was confined in a residential center for the mentally retarded or in state boarding home until 1978. Though a court did give her financial award in compensation, surely nothing can compensate for 42 years of unnecessary and involuntary commitment. Gladys Burr was involuntarily committed by her mother (apparently because of some personality problems) in 1936 at the age of 29. She was diagnosed as psychotic and later declared to be mentally retarded. Though a number of IQ tests administered from 1946 to 1961 showed her to be of normal intelligence, and though a number of doctors stated that she was of normal intelligence and should be released, she was confined in a residential center for the mentally retarded or in state boarding home until 1978. Though a court did give her financial award in compensation, surely nothing can compensate for 42 years of unnecessary and involuntary commitment. |
On a more positive note, with a widely used classification system such as the DSM, individuals with observable sets of symptoms are more likely to receive the same diagnosis across the world and, thus, receive similar treatment. Despite the creation of distinct criteria for each disorder, however, diagnosis is not a clear-cut process. Mental illness may not always present itself consistently throughout the world, and the boundary between normal and abnormal is not always clear.
The DSM, based on descriptions of syndromes, identifies certain critical characteristics of a disorder that have to be met for a diagnosis to be made. The DSM also allows for some non-essential variations. For instance, in the classification of depression, five symptoms must be present, but there are nine symptoms that may be present at once. The DSM details major features of disorders, descriptions of accompanying features, and an account of the onset, course, prevalence, and sex ratio of each disorder. The manual is composed of three main components to assist the clinician: the diagnostic classification, the diagnostic criteria sets, and the descriptive text.
The first component, diagnostic classification, is the list of the mental disorders that are part of the DSM system. Forming a DSM diagnosis involves the selecting of those disorders from the classification that best reflect the signs and symptoms of the patient. The second component, diagnostic criteria, refers to the symptoms that must be present (and for how long) as well as those symptoms that must not be present for an individual to qualify for a specific diagnosis. These diagnostic criteria are useful in that they provide a concise description and summary of each disorder. The last component is the descriptive text associated with each disorder. The descriptive text guides the clinician by systematically describing each disorder under a variety of headings (e.g., diagnostic features, subtypes and/or specifiers, specific culture, age, gender features, and familial pattern).
With each revision of the DSM, clarity was added and validity and reliability were improved. For instance, in the third version of the manual, clinicians were encouraged to consider a wide range of dimensions in forming their assessment. This is referred to as a multiaxial assessment, which allows an individual to be evaluated on five different axes. The first three axes rate the individual’s present condition. The last two axes provide a broader assessment of the specific situation of the individual, one dealing with the stressors that may have contributed to the current illness, and the other dealing with how well the individual has been coping in recent months. Please refer to the table 1, below for a description of each axis.
Table 1: Multiaxial Assessment
| Axis I: Clinical Syndromes |
The clinician checks for the presence or absence of most clinical syndromes (including schizophrenia, mood, anxiety, eating, and sexual disorders). |
| Axis II: Developmental and Personality Disorders |
The clinician looks for the presence or absence of stable, long-term conditions including personality disorders and learning disabilities. |
| Axis III: Physical Conditions |
Relevant information is gathered regarding the individual’s physical health (e.g., presence or absence of a brain tumor). |
| Axis IV: Psychosocial Stressors |
Information regarding psychosocial and environmental problems is obtained. (E.g., a depressed person may find it difficult to recover if he or she does not have supportive friends or family.) |
| Axis V: Global Assessment of Functioning (GAF) |
The clinician rates an individual’s global level of functioning (psychological, social, and occupational) using a scale from 1 to 100. A score of one indicates persistent violence, suicidal behaviour, or inability to maintain personal hygiene. A score of 100 means the person is symptom-free. |
Axis IV and Axis V were added to the third version of the DSM and have the benefit of providing a framework for assessing a person’s life situation and coping skills. Please see table 2 below which highlights Axis IV, and table 3, which describes Axis V (adapted from DSM-III-R).
Table 2: Axis IV scale for rating severity of psychosocial stressors
| Code | Term | Adult Examples | Child or Adolescent Example |
| 1 | None | No apparent psychosocial stressor or enduring circumstances | No apparent psychosocial stressor or enduring circumstances |
| 2 | Mild | Broke up with boyfriend or girlfriend, or child left home; family arguments or job dissatisfaction | Expelled from school or birth of a sibling; chronic parental discord or disabling illness in parent |
| 3 | Moderate | Marriage or marital separation or loss of job; marital discord or serious financial problems |
Expelled from school or birth of a sibling; chronic parental discord or disabling illness in parent |
| 4 | Severe | Divorce or birth of a child; unemployment or poverty | Divorce of parents or unwanted pregnancy; harsh or rejecting parents or multiple foster home placement |
| 5 | Extreme | Death of spouse or serious physical illness diagnosed; victim of rape; ongoing physical or sexual abuse | Sexual or physical abuse or death of a parent; recurrent sexual or physical abuse |
| 6 | Catastrophic | Death of a child, suicide of spouse; hostage or concentration camp experience |
Death of both parents; chronic life threatening illness |
| 0 | Inadequate Information or no change in condition | ||
Table 3: Axis V scale for rating global assessment of functioning
| Code | Description | Example |
| 90 | Good in all areas | Social, occupational (or school), and psychological functioning is without notable problems. Absent or minimal symptoms. |
| 80 | Slight impairment only | Temporary inefficiency in occupation or school work. If symptoms present, they are transient and normal for stressors experienced. |
| 70 | Some difficulty | Despite acceptable overall functioning, person has some problem in social, occupational, or school sphere. Retains some meaningful interpersonal relationships. If present, symptoms are mild. |
| 60 | Moderate difficulty | Social, occupational, or school functioning moderately disrupted, or symptoms of moderate severity, such as occasional panic attacks. |
| 50 | Serious difficulty | Any serious impairment in social, occupational, or school functioning, or serious symptoms such as suicidal ideation or severe compulsive rituals. |
| 40 | Major Impairments | Person shows major impairment in several areas such as work or school, family relationships, judgement, thinking, or mood, or some impairment of reality testing or communication. |
| 30 | Unable to function | Inability to manage in almost all areas; or behaviour considerably influenced by delusions or hallucinations; or seriously impaired judgment or communication. |
| 20 | Some danger | Person’s clinical status judged to be of some danger to self or others; or some failure to maintain minimal standards of personal hygiene; or gross communication impairment. |
| 10 | Persistent danger |
Person judged to be a persistent danger to self or others; or inability to |
To illustrate multiaxial assessment, we can use Trish as an example. Trish is a rather dependent person. She works for a company that just hired an overbearing and authoritarian administrator. As a result of the harsh management practices, Trish has become anxious at work and has experienced an increase in blood pressure. Trish’s diagnosis might be as follows:
|
Axis I: The patient displays general anxiety disorder and has psychological factors that affect her physical condition. Axis II: The patient has dependent personality disorder. Axis III: The patient has hypertension. Axis IV: Level of psychosocial stressors ranks at two (mild). Axis V: Global functioning ranks at 60 (moderate difficulty). |
A more detailed example of multiaxial assessment, summarized from the DSM-III-R Case Book, is presented in the following Case Study. The first part is a description of the patient, and the second part includes a discussion of the diagnosis made by the clinician.
Overanxious Disorder - Case Study 1
|
Description After a year of being overly “nervous”, a 12 year-old girl was brought to a health care practitioner for consultation. The practitioner learned that a year earlier her parents had separated from what seemed to be a rather“stable” marriage. After the separation, the patient began to bite her nails, experience heightened anxiety, and become fearful and apprehensive. She even developed a fear of the dark. She did not have panic attacks but did worry about the safety of her parents. Although her fears were based in reality, they were greatly exaggerated. She also worried about her appearance and often felt awkward and shy. Although she had a couple of close peer relationships, she had difficulty making friends overall. The patient was very tense during the interview – she had sweaty palms and avoided eye contact. When asked if she was sad, she denied it although she admitted she felt somehow responsible for her parents’ separation. Her academic performance was satisfactory, and physical tests showed that she was otherwise healthy. |
Diagnosis The main feature of the patient’s illness is anxiety. Her symptoms do not warrant a phobic disorder, obsessive-compulsive disorder, separation anxiety disorder, or panic disorder diagnosis but rather that of generalized anxiety or overanxious disorder. She worries unrealistically about her parents’ safety, has an inability to relax, is self-consciousness, and is overly concerned about school performance. Her symptoms have persisted for more than six months, thus resulting in the over-anxiety diagnosis. On Axis IV note that the parents’ separation is a moderate psychosocial stressor that relates, most likely, to the development of the Axis I disorder. On the fifth axis, her rating is 65 because she does have close friends and is succeeding at school. The overall diagnosis using the DSM-III-R is as follows: Axis I: Overanxious Disorder Axis II: No Diagnosis or Condition Axis III: None Axis IV: Psychological stressors: Axis V: Global functioning ranks at 65 |
If you are interested in seeing the types of changes that occur when the DSM is updated, refer to the link below which provides a summary of changes that occurred from the DSM-IV-TR to the most recent version of the manual, the DSM-V.
 |
Changes in the DSM-V |
Lesson Review
|
To summarize: • Assessment: collecting information about a patient. |
Assignment
Complete