Lesson 1: Clinical Disorders - Part A
| Site: | MoodleHUB.ca 🍁 |
| Course: | Abnormal Psychology 35 RVS |
| Book: | Lesson 1: Clinical Disorders - Part A |
| Printed by: | Guest user |
| Date: | Thursday, 30 October 2025, 1:14 AM |
Table of contents
- Section/Lesson Objectives
- Introduction
- 1 - Panic Disorder
- 2 - Organic Anxiety Disorder - Case Study 4
- 3 - Obsessive Compulsive Disorder (OCD)
- 4 - Obsessive Compulsive Disorder - Case Study 5
- 5 - Generalized Anxiety Disorder (GAD)
- 6 - Phobias
- 7 - Simple Phobia - Case Study 6
- 8 - Eating Disorders
- 9 - Anorexia and Bulimia - Case Study 7
- 10 - Pica - Case Study 8
- 11 - Impulse Control Disorders
- 12 - Kleptomania - Case Study 9
- 13 - Pyromania - Case Study 10
- 14 - Trichotillomania - Case Study 11
- Lesson Review
- Assignment
Section/Lesson Objectives
The student will ...
• Understand and describe the general symptoms of the clinical disorders discussed in the course [This lesson]
• Discuss the possible causes of clinical disorders [This lesson]
• Understand and describe the general symptoms of the cognitive disorders discussed in the course
• Discuss the possible causes of cognitive disorders
• Understand and describe the general symptoms of intellectual disability
• Discuss the possible causes of intellectual disability
• Understand and describe the general symptoms of the personality disorders discussed in the course
• Discuss the possible causes of personality disorders
Introduction
In the lesson content you will come across some terms in maroon color that are bolded. Look them up in the course Glossary.
Mental disorders are illnesses that involve the brain. Because of this, the way people think and behave are affected to varying degrees. People who have mental disorders find that their sense of well-being has been compromised. They may have problems both at home and at work. A combination of genetics, environment, social factors, cultural factors, and physical health work together to make us who we are at any given time. Thankfully, many disorders can be treated effectively – with patients leading full lives after treatment.
Mental disorders are associated with disturbances in six primary domains of brain function.
Figure 1: Mental Disorders
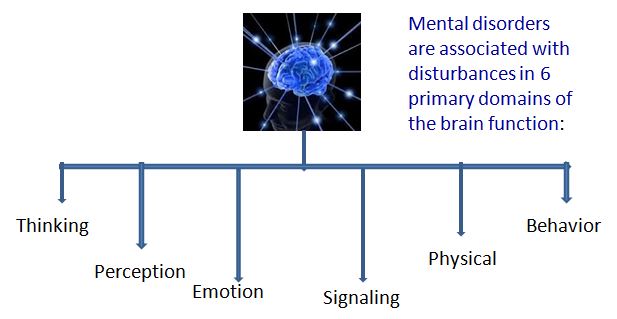
When the brain is not functioning properly in one or more of its six domains, and a person experiences problems that interfere with his or her life in a significant way, they may have a mental disorder. (Note: signaling means being responsive and reacting to the environment.) However, it is important to note that not all disturbances of brain functioning are mental disorders. Some can be a normal or expected response to the environment -- for example: grief when somebody dies or acute worry, sleep problems and emotional tension when faced with a natural disaster such as a hurricane.
What is the difference between mental distress and mental disorders?
| Distress | VS.
|
Disorders |
|
Common; caused by a problem or event; usually not severe (may be severe); usually short lasting ; professional help not usually needed; professional help can be useful; DIAGNOSIS NOT NEEDED. |
Less common; may happen without any stress; often with high severity; usually long lasting; professional help usually needed. NEEDS TO BE DIAGNOSED. |
What causes mental illness?
A variety of different insults to the brain can lead to mental illness. Basically there are TWO major causes that can be independent or can interact. They are
|
GENETICS (the effect of genes on brain development and brain function) and ENVIRONMENT (the effect of things outside the brain on the brain -- such as infection; malnutrition; severe stress etc.) |
|
|
|

Although mental illness may be classified in various ways, for the purpose of this course, mental disorders shall be divided into four broad categories, each of which can be divided into many sub-categories.
Please see Figure 2.
Figure 2: Mental Disorders

Clinical Disorders
Applying the categorization scheme in Figure 2 more than 12 broad sub-groups can be ascribed to the main category of clinical disorders. The first sub-group is anxiety disorders that include such conditions as panic disorder, post-traumatic stress disorder (PTSD), obsessive compulsive disorder (OCD), generalized anxiety disorder (GAD), phobias, and more. The second sub-group relates to adjustment disorders and the third, dissociative disorders. The fourth sub-group deals with eating disorders such as pica, anorexia nervosa, and bulimia nervosa. The fifth sub-group deals with factitious disorder. The remaining sub-groups deal with impulse control (e.g., kleptomania, trichotillomania, pyromania), mood disorders (e.g., depression, bipolar disorder, dysthymic disorder) schizophrenia and psychosis, sleep disorders, sexual and gender identity disorders, somatoform disorders, and substance-related disorders. This course will describe only a small fraction of the various clinical disorders.
PART A
Panic Disorder
Individuals experiencing this disorder suffer from unexpected attacks of anxiety that develop abruptly and reach a critical point within a short period of time (often between two and ten minutes.) These periods of intense fear and discomfort involve at least four of the following symptoms which peak within 10 minutes.:
|
Symptoms • heart palpitations or a “pounding” heart |
 People with Panic Disorder experience recurrent, unexpected panic attacks and they greatly fear having another attack. This concern and worry is part of the diagnosis of panic disorder. Some individuals may become afraid to leave the house (agoraphobia) to avoid triggering another attack. Some may fear they are "losing their mind" or feel they are going to die. For a panic disorder diagnosis, a person must experience at least four attacks in one month or fewer attacks accompanied by extreme fear of recurrence.
People with Panic Disorder experience recurrent, unexpected panic attacks and they greatly fear having another attack. This concern and worry is part of the diagnosis of panic disorder. Some individuals may become afraid to leave the house (agoraphobia) to avoid triggering another attack. Some may fear they are "losing their mind" or feel they are going to die. For a panic disorder diagnosis, a person must experience at least four attacks in one month or fewer attacks accompanied by extreme fear of recurrence.
Many individuals experience panic attacks during periods of high stress. Most, however, resume normal  functioning without further incident. Only a very small portion of the population develop panic disorder. Some statistics say 2-3% of the general population are affected - slightly more females than males. The onset of panic disorder is commonly between the ages of 15-25. People who have parents with panic disorder have an eight times higher risk of also developing panic disorder themselves. To summarize, people with panic disorder have the following symptoms: a sense of impending doom and worry, difficulty breathing (in addition to many other physical symptoms), and a desire to escape or avoid people, places, and events that produce anxiety. Like all anxiety disorders, panic disorder can grow progressively worse if not treated. Please read Case Study Four that combines a review of panic disorder with a unique biological causal factor!
functioning without further incident. Only a very small portion of the population develop panic disorder. Some statistics say 2-3% of the general population are affected - slightly more females than males. The onset of panic disorder is commonly between the ages of 15-25. People who have parents with panic disorder have an eight times higher risk of also developing panic disorder themselves. To summarize, people with panic disorder have the following symptoms: a sense of impending doom and worry, difficulty breathing (in addition to many other physical symptoms), and a desire to escape or avoid people, places, and events that produce anxiety. Like all anxiety disorders, panic disorder can grow progressively worse if not treated. Please read Case Study Four that combines a review of panic disorder with a unique biological causal factor!
For a diagnosis of panic disorder, a patient must have:
1. Recurrent unexpected panic attacks
2. One or more of the attacks have been followed by > 1 month of:
- Worry about the implications of the attack or its consequences
- A significant change in behaviour as a result of the attacks
- Persistent concern of having additional attacks
3. Can be +/- agoraphobia
4. Panic attacks are not due to substance abuse, medications or a general medical condition.
5. Panic attacks are not better accounted for by another mental disorder.
To learn more about panic disorder, click on the link below:
|
Teen Mental Health http://teenmentalhealth.org/learn/mental-disorders/panic-disorder/ |
PART A
Organic Anxiety Disorder - Case Study 4
|
Description A 78 year-old retired president of a lumber company presented During the assessment of his symptoms, the patient denied that he had laboured breathing, heart palpitations, nausea, and choking sensations, but admitted that he did have trembling, sweating, light-headedness, and a fear that he would die if he did not get outside. The patient reported that he had a need to be “active.” Upon further investigation by the doctor, the man remembered a similar series of episodes almost thirty years earlier following eye surgery. The patient was confined to his bed for days with eye patches and an apparatus to prevent head movement. Once the confinement was over, the patient experienced the recurring symptoms for more than a year. The retired lumberman said that he was sleeping and eating well and had not gained or lost weight. He told the doctor that he did not have crying spells, urinary incontinence (loss of bladder control), or a decrease in energy. He did state that he had been taking Valium each day (5 to 10 mg) for the last two months to help decrease feelings of nervousness and tension. He also noted mild memory problems, some difficulty with balance, and pain in his right arm. His difficulty with balance prevented him from summer gardening as did his difficulty with the co-ordination of brisk walking and other movement. He was also found to have a “beefy” red tongue which gave him considerable discomfort. A medical examination discovered a form of anemia (macrocytic) and a vitamin B12 deficiency. The patient was given a B12 replacement that effectively stopped his panic attacks. |
Diagnosis The patient described symptoms typical of panic disorder; however, laboratory findings showed a vitamin B12 deficiency. Consequently, a diagnosis of organic anxiety disorder was made because the B12 replacement therapy effectively stopped the episodes. Regarding the episodes of panic earlier in his life (in the absence of a known organic cause), it is assumed that he then had panic disorder. The current organic anxiety disorder may be a manifestation of an underlying vulnerability to panic attacks. See below for a DSM summary. Axis I: Organic Anxiety Disorder Axis II: No diagnosis or condition Axis III: Vitamin B12 deficiency Axis IV: Severity: 1 – none Axis V: Current GAF: 0 |
 himself for treatment following a series of episodes in which he felt apprehensive and restless. To decrease his feelings of discomfort, he insisted upon being outdoors. He described his most recent episode as occurring at 3:00 a.m., a week prior to seeing the doctor. He awoke from his sleep with a feeling that the walls were coming in on him. He claimed he was fully awake; he got up, dressed himself, and went outside. He felt much better once outdoors, but he claimed it took an entire day to feel “normal” again.
himself for treatment following a series of episodes in which he felt apprehensive and restless. To decrease his feelings of discomfort, he insisted upon being outdoors. He described his most recent episode as occurring at 3:00 a.m., a week prior to seeing the doctor. He awoke from his sleep with a feeling that the walls were coming in on him. He claimed he was fully awake; he got up, dressed himself, and went outside. He felt much better once outdoors, but he claimed it took an entire day to feel “normal” again. PART A
Obsessive Compulsive Disorder (OCD)
 This disorder can evolve into one of the more severe of the anxiety disorders. People with OCDs are bombarded with persistent and uncontrollable thoughts, as well as compulsions to perform specific actions over and over again. The obsessive part of the disorder involves recurrent and intrusive thoughts or images that cause elevated anxiety. The compulsive part of the disorder requires the person to perform repetitive behaviours or mental acts to help reduce the anxiety caused by the obsession. Examples of these are counting, touching, washing and checking.
This disorder can evolve into one of the more severe of the anxiety disorders. People with OCDs are bombarded with persistent and uncontrollable thoughts, as well as compulsions to perform specific actions over and over again. The obsessive part of the disorder involves recurrent and intrusive thoughts or images that cause elevated anxiety. The compulsive part of the disorder requires the person to perform repetitive behaviours or mental acts to help reduce the anxiety caused by the obsession. Examples of these are counting, touching, washing and checking.
|
Symptoms • heart palpitations or a “pounding” heart |
 People with OCD spend a minimum of one hour each day engaging in their particular compulsion. Interestingly enough, most people experience the same kinds of thoughts, but only specific individuals experience them differently. When such people try to fight these normal thoughts, their frequency increases, which causes heightened anxiety. If not effectively treated, OCD can persist through a person’s life. The individual who suffers from an OCD essentially becomes trapped in a pattern of repetitive thoughts and senseless behaviours that are distressing and extremely challenging to overcome.
People with OCD spend a minimum of one hour each day engaging in their particular compulsion. Interestingly enough, most people experience the same kinds of thoughts, but only specific individuals experience them differently. When such people try to fight these normal thoughts, their frequency increases, which causes heightened anxiety. If not effectively treated, OCD can persist through a person’s life. The individual who suffers from an OCD essentially becomes trapped in a pattern of repetitive thoughts and senseless behaviours that are distressing and extremely challenging to overcome.
OCD often begins in adolescence or early adulthood, although it can start in childhood. It is quite common and affects both men and women. Those with OCD are at higher risk for developing depression and other anxiety disorders. OCD whould not be confused with superstitions or those repetitive checking behaviors that are common in everyday life. They are not simply excessive worries about real life issues. A person with OCD will have significant symptoms of either obsessions or compulsions or both. These symptoms will be severe enough to cause marked distress, are time consuming (take up more than one hour per day) and significantly interfere with a person's normal activities, (work, school, social, family, etc.).
Please read Case Study Five.
Click on the link below to learn more about OCD:
|
Teen Mental Health http://teenmentalhealth.org/learn/mental-disorders/obsessive-compulsive-disorder-ocd/ |
PART A
Obsessive Compulsive Disorder - Case Study 5
|
Description At an interview, a 14 year-old girl was recalling how her life was just one year earlier. As a 13 year-old, she was obsessed with germs. She was afraid they were all over her clothes and other belongings. She shook the germs from her clothes for thirty minutes before wearing them. She would wash her hands before washing her face. She would then wash her hands again before getting dressed. At her worst point, she used rubbing alcohol for washing – this caused her hands to bleed. These rituals often left no time for breakfast before going to school. At the most severe point with the disorder, she had to get up at 6:00 a.m. just to get ready for an event at 11:00 a.m., but her disorder was so severe that, on occasion, even five hours were insufficient to prepare to leave the house. The teen also had some obsessions and compulsions regarding numbers. For example, she would often re-read things three times. She would also mentally say “three” (or a multiple of three) to “clean” germs from “dirty” words. In one day she might say a multiple of three over 124 times! She was very much afraid that something bad would happen if she did not perform her rituals – although her friends told her that the behaviour was “stupid,” to which she agreed. She even began worrying that something bad would happen to her family if she did not perform her rituals. After treatment, the girl was much better. On occasion, she still reads things three times if she has trouble understanding the content the first time, but she is able to get up, brush her teeth, shower, and get dressed in half an hour! |
Diagnosis The girl vividly displays symptoms of severe obsessive compulsive disorder. Her obsessions and compulsions are a major source of stress to her and interfere with her daily functioning. Her obsessions are based on ideas that interject themselves into her consciousness and are experienced as senseless. Her need to neutralize such thoughts has led to repetitive and persistent compulsions. For example, washing hands for hours at a time to prevent infection by germs (to the point that her hands were bleeding) was clearly excessive. She reacted as though the dangers were real despite knowing they were not. While she does display evidence of OCD, she does not display obsessive compulsive personality disorder – a disorder that involves such traits as perfectionism, indecisiveness, and a restricted ability to express warm and tender emotions. She did, however, admit to an episode of major depression – a common occurrence with OCD sufferers. Her DSM diagnosis for Axis I is obsessive compulsive disorder - Severe |
The Hollywood movies “Matchstick Men” and “As Good as it Gets” both have leading characters with OCDs.
PART A
Generalized Anxiety Disorder (GAD)
This common anxiety disorder affects approximately one in four people at some point. The characteristic feature of this disorder is excessive worry on most days. This causes distress and/or functional impairment to the person. An individual may worry about work, relationships, health, approval, goals, or money.
Worry or concern is a normal part of our lives. When worry becomes disturbing and troublesome, people may become restless, fatigued, and irritable. They may experience inability to concentrate, have impaired sleep, and feel muscle tension. For a GAD diagnosis, people must have difficulty controlling their worry and at least six of the symptoms listed in Table 5.1 (Carson et al, 1988). Such criteria must be present for at least six months.
Table 5.1:
Symptoms of Generalized Anxiety Disorder
- trembling, twitching, “shaky”
- muscle tension, aching, sore
- restlessness
- easily fatigued
- “keyed up”, “on edge”
- exaggerated startle response
- difficulty sleeping
- concentration difficulties
- irritability
- shortness of breath, “smothering”
- rapid pulse, palpitations
- sweating, clammy hands
- dry mouth
- dizziness, light-headedness
- nausea, diarrhea, or other gastrointestinal distress
- hot flashes or chills
- frequent urination
Watch the video below about Connor's experience with GAD and OCD.
What are the criteria for the diagnosis of GAD?
1. Excessive anxiety and worry occurring for at least 6 months about several things
2. Difficulty controlling the worry.
3. The anxiety and worry are associated with 3 or more of the following: restlessness or feeling on edge, fatigued, difficulty concentrating, muscle tension or sleep disturbance.
4. Anxiety and worry are not due to substance abuse, a medical condition or a mental disorder.
5. The anxiety and physical symptoms cause marked distress and significant impairment in daily functioning.
Treatment:
Some people with GAD will experience improvements in their anxiety and functioning with supportive cognitive based counselling. Others may require medication. Referral to an appropriate health professional for medical attention could be considered if the GAD is severe and if the functional impairment is extensive. For some, merely knowing that they have GAD and receiving supportive counseling may be helpful enough.
*Some people with GAD may go on to develop a clinical depression. Some people may begin to use substances such as alcohol to help control their anxiety. If this occurs, they may be at risk of developing a substance abuse or substance dependence problem.
Read more about generalized anxiety disorder at the web site below:
|
Teen Mental Health http://teenmentalhealth.org/learn/mental-disorders/generalized-anxiety-disorder/ |
PART A
Phobias
 Fear, in general, is beneficial. It helps protect people from otherwise dangerous and life-threatening situations. For example, a fear of food poisoning contracted from ingesting raw meat products may make a person fully cook his or her pork roast. A fear of brain damage may persuade people to wear bicycle helmets when cycling. A fear of bears may encourage hikers to hike in groups and carry bear spray. Phobias, however, involve intense and irrational fears. People can fear a particular thing, place, or condition. Social phobia, a common affliction, involves overwhelming and excessive self-consciousness in everyday social situations. Affected individuals are fearful of being observed and judged by others and of being embarrassed or disgraced by their own actions. Such individuals are likely to avoid public speaking, meeting new people, or using public washrooms.
Fear, in general, is beneficial. It helps protect people from otherwise dangerous and life-threatening situations. For example, a fear of food poisoning contracted from ingesting raw meat products may make a person fully cook his or her pork roast. A fear of brain damage may persuade people to wear bicycle helmets when cycling. A fear of bears may encourage hikers to hike in groups and carry bear spray. Phobias, however, involve intense and irrational fears. People can fear a particular thing, place, or condition. Social phobia, a common affliction, involves overwhelming and excessive self-consciousness in everyday social situations. Affected individuals are fearful of being observed and judged by others and of being embarrassed or disgraced by their own actions. Such individuals are likely to avoid public speaking, meeting new people, or using public washrooms.
With specific phobias, exposure to the feared object, place, or condition almost always triggers an anxiety response, often in the form of a panic attack. Although adults with phobias generally understand that their fear is unreasonable, some children do not. Individuals with phobias tend to avoid the feared object or situation. In some cases where this is not possible (such as getting an injection when you have a fear of needles), a person will endure the situation with intense discomfort. The avoidance of specific objects, places, or conditions, however, may interfere with an individual’s normal routine and functioning. People may not leave their houses in their determination to avoid certain triggers.
For a diagnosis of a specific phobia, the fear and anxiety related to an object or situation cannot  be due to another psychological disorder and, for those under 18, the fear has to be present for at least six months.
be due to another psychological disorder and, for those under 18, the fear has to be present for at least six months.
Phobias may develop for a number of reasons. If a father, for example, has an irrational fear of insects, he may pass this fear to his child through the child’s observation of the father’s avoidance behaviours and reactions when encountering an insect.
People may also develop a phobia relating to a traumatic event. For example, if they almost drowned during childhood, they may avoid all activities that involve water. They would not water-ski, canoe, fish, swim, etc. A third way to develop a phobia is through misinterpretation of information. A person who reads about negative experiences with dentists and speaks with people regarding their poor dental work may develop an irrational fear of all dentists, dentist offices, and dental tools. The sight of a dentist’s drill may elicit a panic attack severe enough to prevent a person from getting a simple dental checkup!
Read more about social phobias the web site below:
|
Teen Mental Health http://teenmentalhealth.org/learn/mental-disorders/social-anxiety-disorder/ |
Watch the video below which provides a summary of panic disorders, OCD, generalized anxiety disorder and phobias.
PART A
Simple Phobia - Case Study 6
|
Description Voluntarily seeking treatment, a 28 year-old computer programmer describes fears that prevent him from going to see his terminally ill father-in-law in the hospital. He explains that he is afraid of situations relating to bodily injury or illness. He does not like to have a blood sample taken or to see or hear about sick people. He does not seek medical treatment when he is sick nor does he visit sick friends or family members. He avoids listening to descriptions of medical procedures, bodily trauma, or disease. He even became a vegetarian to avoid thinking about killing animals. When the programmer was nine years-old, his Sunday school teacher gave a descriptive account of a leg operation. As the teacher spoke, the patient began to feel anxious and light-headed. He then began to sweat profusely until he fainted. He also told of his dislike of vaccinations and other regular medical procedures throughout his school career. He recounted frequent fainting episodes and near-fainting episodes whenever he saw a sick or disfigured person. Even into adulthood, he would faint if he observed the slightest physical wound or heard of an injury or illness. He told the doctor of his recent encounter in a store with someone who was confined to a wheelchair. He started to wonder if the person was in pain – so much so that he became distressed and fainted. He was very embarrassed when he regained consciousness. The patient described no other emotional problems, enjoyed work, had a good marriage, and had many friends. |
Diagnosis The computer programmer had a fear of thinking about or being near any situation involving physical injury or illness. While he continued to avoid situations that may elicit an episode of fainting, he acknowledged that his fear was irrational. Although the avoidance behaviour did not appear to affect his normal routines and social life, he was distressed about his fear and wished to rectify the situation. The programmer did not have an obsession regarding germs, so an OCD diagnosis was not warranted. Post-traumatic stress disorder was also not implied because he did not observe mutilation or injury on the battlefield. The diagnosis, therefore, was simple phobia - specifically, a blood-injury phobia. Like many others who have this phobia, the patient felt faint in the presence of the phobic stimulus. His DSM diagnosis for Axis I is simple phobia.
|

PART A
Eating Disorders
Video: Eating Disorders
<
 In western society the prevalence of eating disorders is greater than in most other parts of the developed world. Eating disorders can take several forms: bulimia nervosa, anorexia nervosa, binge-eating disorder, and pica. In each of these disorders, individuals do not have a healthy relationship with food. In North America, much media coverage is given to both anorexia nervosa and bulimia nervosa.
In western society the prevalence of eating disorders is greater than in most other parts of the developed world. Eating disorders can take several forms: bulimia nervosa, anorexia nervosa, binge-eating disorder, and pica. In each of these disorders, individuals do not have a healthy relationship with food. In North America, much media coverage is given to both anorexia nervosa and bulimia nervosa.
With anorexia, a disorder first described over three hundred years ago, the patient experiences unhealthy and rapid weight loss. Afflicted individuals also have excessive concern with body shape and mass, are preoccupied with food and calories, and often have ritualized eating and food preparation habits. Individuals may skip meals, only eat certain foods, abuse laxatives, and exercise excessively. Body weight drops 15% below that considered healthy, and many individuals experience hair loss on their heads and hair growth elsewhere. In severe cases, the brain shrinks as the body, starving for nutrients, uses the fatty sheath surrounding nerve cells for energy. Thought processes are negatively affected and often a secondary addiction (such as compulsive shopping or alcohol abuse) accompanies this disorder as do various physical complications. Please refer to List 8.1 for a partial review of medical problems.
List 8.1:
Complications Resulting from Anorexia Nervosa
| - slow or irregular heart rate - heart failure - hypoglycemia - fluid in the sac enclosing the heart - amenorrhea (missing 3 consecutive periods) - lack of sexual interest or impotence - swelling of the salivary glands - stomach expansion |
- weakness - yellowing of the skin - dehydration - anemia - tooth decay - constipation - hypothermia - kidney damage |
The media can have a huge impact on the average person's self esteem, as magazines and movies usually portray beautiful individuals; many of whom are very thin. This can distort the image that we have of ourselves and make us feel fat, when in fact, you may be a healthy weight.
Watch this video that shows how the media can have an impact:
Barbie dolls have been around for generations of young women. As a result, her sleek figure can stick with young girls that think this is what beautiful looks like. However, in reality if we took Barbie's proportions and made a life-size Barbie, it would be a freakish woman with pencil-thin legs, breasts that threaten to
topple her over, and a body mass index that would put her in the anorexic range. Unfortunately, this is the role model that many young girls believe is beautiful.
young girls that think this is what beautiful looks like. However, in reality if we took Barbie's proportions and made a life-size Barbie, it would be a freakish woman with pencil-thin legs, breasts that threaten to
topple her over, and a body mass index that would put her in the anorexic range. Unfortunately, this is the role model that many young girls believe is beautiful.
Video: Amy's experience with anorexia.
 In cases of bulimia, sufferers are preoccupied with body image and body mass. An individual consumes massive amounts of food only to find a way to purge the calories from his or her body by vomiting, compulsively exercising, using diuretics, or abusing laxatives. A person with bulimia can be overweight, underweight, or of normal weight. Like those with anorexia, many patients with bulimia have secondary addictions. Some common complications from bulimia include tooth decay, enlarged heart, electrolyte imbalance, renal complications, dehydration, and kidney disease. For a DSM diagnosis, individuals must have a minimum of two binges per week for three months. Binging is most often done in secret where individuals consume an excessive amount of food (upwards of 20 000 calories per episode) followed by purging behaviour.
In cases of bulimia, sufferers are preoccupied with body image and body mass. An individual consumes massive amounts of food only to find a way to purge the calories from his or her body by vomiting, compulsively exercising, using diuretics, or abusing laxatives. A person with bulimia can be overweight, underweight, or of normal weight. Like those with anorexia, many patients with bulimia have secondary addictions. Some common complications from bulimia include tooth decay, enlarged heart, electrolyte imbalance, renal complications, dehydration, and kidney disease. For a DSM diagnosis, individuals must have a minimum of two binges per week for three months. Binging is most often done in secret where individuals consume an excessive amount of food (upwards of 20 000 calories per episode) followed by purging behaviour.
Like anorexia and bulimia, binge-eating disorders are more prevalent in women than men. Men, however, can make up 25% of binge-eaters. People suffering from this disorder are often overweight because they do not regularly fast, excessively exercise, or purge to control their weight. Some individuals continually eat throughout the day with no specific meal time while others have large binges in response to stress or anxiety. Similar to anorexia and bulimia, this disorder is often co-morbid with depression. Some research indicates a possible genetic link predisposing individuals to eating disorders. Popular culture suggests the increase of these disorders may be due in part to sociocultural factors (e.g., television, models, family dynamics) and/or sexual abuse. This research has yet to be substantiated.
Video: Demi Lovato talks about her eating disorder
Following are two case studies regarding eating disorders, the second of which describes pica. Pica is an eating disorder where non-food items (e.g., chalk, sawdust, paperclips) are ingested. Individuals have an abnormal desire to eat substances not normally eaten.
PART A
Anorexia and Bulimia - Case Study 7
|
Description After watching a television show relating to Despite how she looked to others, the patient never felt happier about her appearance. She was flat everywhere and each rib and back vertebra could be seen when she bent over. The more weight she lost, the more worried she became about becoming fat. She was afraid of drinking water for days at a time because it added pounds on the scale. She did drink, however, to help her vomit after a binge. Binging was so successful that she stopped using the laxatives despite complaining of constipation. In fact, the mere sight of laxatives made her nauseated. The patient exercised for many hours each day to tone her figure. She even joined the college track team, but she had to quit because she could not complete one lap. She vomited before practice which made her too dizzy to run. At this time she had not menstruated in two years. During her last semester before she dropped out of college she read an article on anorexia nervosa. The article scared her into trying to eat and digest healthy food. While she loathed eating nutritious food items, she forced herself to do so and accepted a new attitude regarding food. At 5’6” and fighting panic, she inched her weight to a range of 105 and 115 pounds. She would only eat nutritious food (no junk food or sweets) but became reclusive in her home as she was embarrassed to be “so fat.” She also began to push away friends and activities that used to make her life complete. The patient, however, was able to hold a job despite binging, purging, and feeling sick all the time. Her binging and purging was harder to perform each time, and the act took longer to complete. She needed to use different instruments (e.g., electric cords) to help her vomit as well as six to ten doses of ipecac (a substance that induces vomiting). Her knees became calloused from the time she spent kneeling while throwing up. Sometime a session of vomiting would last two to three hours but could also last as long as eight hours. A vomiting session left her dehydrated, cold, and shaking with broken blood vessels in her eyes. In her letter to the treatment centre, the patient described her desire to break free from her overwhelming eating disorder. She cried for help from behaviours such as isolation, taking Aspirin® for the pain in her hands, taking potassium supplements (to counteract the diuretics she took), shoving cords down her throat, and spending hours heaving into the toilet. It was easily decided that she was a suitable candidate for treatment. Upon her inclusion in the treatment program it was learned that her eating disorder began during her teen years. At 14 years-old, and at her adult height of 5’6”, she believed she was fat at 128 pounds. She began to diet, unsuccessfully, soon reaching 165 pounds. Not wanting to gain any more weight, she began to diet seriously and dropped to 130 pounds. At this time she felt depressed, overwhelmed, and insignificant. She also wanted to maintain an “A” average at school, so she avoided difficult classes and began to lie to avoid humiliation. She had extreme anxiety regarding the opposite sex and thus transferred to a girls’ school for her last year of high school. As attested to in her letter, her eating and dieting became drastically worse in college. Although she decided to gain weight from her low of 88 pounds, her binging and purging got worse and she dropped out of college. The patient is the only daughter of four children. She comes from an upper-middle-class family with an alcoholic father. The parents have a strained relationship, and the relationships between her parents and her brothers are strained. No other family member has had psychiatric treatment. |
Diagnosis The patient obviously displayed the features of anorexia nervosa. She had an intense and irrational fear of becoming fat although she was dramatically underweight. Her self-perceived body image was so unrealistic that while she thought she was fat, others thought she was normal. When she thought she was beautiful, others saw a grotesquely thin skeleton. Despite being hungry, the woman lost 30% of her body weight through dieting, vomiting, excessive exercise, and the use of drugs. This information resulted in a diagnosis of anorexia nervosa. Because she also binged and purged at least twice a week for three months, the additional diagnosis of bulimia nervosa was made. Her DSM diagnosis is as follows: Axis I: Anorexia Nervosa, Severe Follow Up During her treatment the patient was able to give up diuretics and other medication completely. After returning home, she continued psychiatric treatment for about six months until her family withdrew their support. During that period she had made some progress, but she was unable to change most of her behaviour. Two years after leaving treatment, she wrote to the hospital saying that she was “much better”, that she had returned to college and was seeing a nutritionist and counsellor. Her weight was normal and she was menstruating regularly despite the occasional episode of binging and purging. She was no longer using diuretics or laxatives.
|
 eating disorders, a 23 year-old woman requested admittance to the treatment program highlighted on the TV show. To be admitted, she had to describe her eating behaviour. She began her story describing her desire to lose weight in college. She started to use a few laxatives but, with continued use, her current dose became ineffective. She gradually increased the dosage until she was taking 250-300 pills at one time, downing 20 pills with one swallow of water. She lost weight – as much as 20 pounds in a 24-hour period (mostly water), but became so dehydrated that she could not stand and could barely talk. Sometimes the woman would not eat for days. Then, with the first bite of food, she would be so overcome with guilt and hunger that she would binge. After speaking with a friend from the same dormitory at college, she learned that vomiting after the binges would prevent weight gain. She learned that she could eat large amounts of food, then induce vomiting, and still lose weight. Her weight dropped to 90 pounds. At this time her hair started to come out in handfuls and her teeth were loose.
eating disorders, a 23 year-old woman requested admittance to the treatment program highlighted on the TV show. To be admitted, she had to describe her eating behaviour. She began her story describing her desire to lose weight in college. She started to use a few laxatives but, with continued use, her current dose became ineffective. She gradually increased the dosage until she was taking 250-300 pills at one time, downing 20 pills with one swallow of water. She lost weight – as much as 20 pounds in a 24-hour period (mostly water), but became so dehydrated that she could not stand and could barely talk. Sometimes the woman would not eat for days. Then, with the first bite of food, she would be so overcome with guilt and hunger that she would binge. After speaking with a friend from the same dormitory at college, she learned that vomiting after the binges would prevent weight gain. She learned that she could eat large amounts of food, then induce vomiting, and still lose weight. Her weight dropped to 90 pounds. At this time her hair started to come out in handfuls and her teeth were loose.PART A
Pica - Case Study 8
|
Description A small five year-old boy was admitted to |
Diagnosis The eating of non-nutritive non-food items can be seen in other disorders such as autism, schizophrenia, and Klein-Levin syndrome. When there are no other symptoms of such disorders, a diagnosis of pica is made. Pica is often associated with a common history in the mother and low socioeconomic status – much like this case. The DSM diagnosis for Axis I is pica. |
 hospital for nutritional anemia, the cause of which appeared to be his ingestion of paint, plaster, dirt, wood, and paste. He began adding non-food items to his diet at 19 months of age when he ingested lighter fluid. The patient came from a poor welfare family – his parents were young, immature, and dependent. He was the result of the unplanned pregnancy to a 16 year-old mother. Although his mother began eating dirt when she was pregnant, the pregnancy itself was uneventful. His father periodically used drugs and alcohol.
hospital for nutritional anemia, the cause of which appeared to be his ingestion of paint, plaster, dirt, wood, and paste. He began adding non-food items to his diet at 19 months of age when he ingested lighter fluid. The patient came from a poor welfare family – his parents were young, immature, and dependent. He was the result of the unplanned pregnancy to a 16 year-old mother. Although his mother began eating dirt when she was pregnant, the pregnancy itself was uneventful. His father periodically used drugs and alcohol.PART A
Impulse Control Disorders
Many psychological problems are characterized by a loss or lack of control in certain situations (such as OCD, alcoholism). The factor that makes impulse control disorder different from other disorders is a lack of other maladaptive thoughts and actions. With an impulse control disorder (ICD), a person cannot resist and will act on an impulse that is potentially harmful. All individuals with ICD have tension in common. Tension builds to an irresistible level that triggers action on the part of the individual. The action brings about a feeling of relief or pleasure and, on occasion, guilt or remorse.
 Three well-known ICDs are kleptomania, pyromania, and trichotillomania. The first, kleptomania, differs from theft in that the individual taking the item does not need the item for its monetary value or practical use, and most often, items are not taken as an expression of anger or revenge. Before the theft, the individual feels rising tension, but after, the individual has a sense of pleasure followed by regret. People who steal as a career are generally not kleptomaniacs. Those individuals who steal because they have no regard for the law may have conduct disorder (if children) or antisocial personality disorder (if adult). Those individuals who steal out of need or desperation (adjustment disorder) or to support an addiction (substance abuse disorder) are not considered kleptomaniacs. Some kleptomaniacs, in fact, steal the same type of item over and over again – and sometimes the item is relatively worthless! Overall, true kleptomania is a somewhat rare problem that affects more women than men. Individuals do not want to steal, but they must as a way to relieve anxiety and obtain temporary gratification.
Three well-known ICDs are kleptomania, pyromania, and trichotillomania. The first, kleptomania, differs from theft in that the individual taking the item does not need the item for its monetary value or practical use, and most often, items are not taken as an expression of anger or revenge. Before the theft, the individual feels rising tension, but after, the individual has a sense of pleasure followed by regret. People who steal as a career are generally not kleptomaniacs. Those individuals who steal because they have no regard for the law may have conduct disorder (if children) or antisocial personality disorder (if adult). Those individuals who steal out of need or desperation (adjustment disorder) or to support an addiction (substance abuse disorder) are not considered kleptomaniacs. Some kleptomaniacs, in fact, steal the same type of item over and over again – and sometimes the item is relatively worthless! Overall, true kleptomania is a somewhat rare problem that affects more women than men. Individuals do not want to steal, but they must as a way to relieve anxiety and obtain temporary gratification.
Pyromania is a psychological problem that involves setting fires for pleasure. The individual experiences a  sense of relief or gratification from the experience. Pyromania differs from arson in that the individual does not set fires for financial gain, to hide criminal activity, or to express anger. If setting fires is a part of another disorder (conduct disorder or bipolar disorder), then pyromania is not diagnosed. In general, pyromania is a rare problem in which the individual has an unusual and uncontrollable fascination with fire.
sense of relief or gratification from the experience. Pyromania differs from arson in that the individual does not set fires for financial gain, to hide criminal activity, or to express anger. If setting fires is a part of another disorder (conduct disorder or bipolar disorder), then pyromania is not diagnosed. In general, pyromania is a rare problem in which the individual has an unusual and uncontrollable fascination with fire.
Another rare ICD is trichotillomania. Individuals suffering from this disorder pull out their own hair in an habitual fashion while experiencing tension relief and/or pleasure. For a trichotillomania diagnosis to be made, the noticeable hair loss that results must not be due to underlying medical conditions. The disorder must also result in clinical distress or impairment in life functioning. Please read the next three case studies.
PART A
Kleptomania - Case Study 9
|
Description A 34 year-old woman came for counselling regarding problems in her marriage. She was wealthy and she had married a successful businessman. She felt her husband was demanding and insensitive; he accused her of being a self-centred compulsive liar. During their marriage, each partner had numerous affairs, which each confessed to, and both partners resolved to stop. The affairs, however, would eventually begin again, on and off, for most of their ten-year marriage. The woman also described a special problem that caused her much concern. She had urges to go to expensive clothing stores and steal an item of clothing. Without her husband’s knowledge, she had over the last few years stolen several items. Although she had more than enough money to buy the items, she rarely stole expensive items. Some stolen items she did not even wear. She realized that her behaviour was irrational. The patient would become aware of a craving to steal several days before she went “shopping.” Gradually, the desire built in her mind until, impulsively, she walked into a store and stuffed an item of clothing under her coat or in a bag. Once she was safely out of the store, she experienced a great sense of relief and contentment. When she arrived home, however, she felt tense and guilty. She also told the doctor about how successful and accomplished she was – that she was superior, beautiful, and talented. She also noted that her husband was handsome, aggressive, and successful – a perfect match for her. Because their marriage was not trouble-free, she decided that it was due to her husband’s unreasonable expectations of her and his not spending enough time with her. She did, however, confess to telling “white lies” to her husband instead of admitting that she had done something “stupid.” |
Diagnosis While the reason for seeking treatment was marital difficulties, the information makes obvious that the woman was a kleptomaniac. She could not resist the urge to steal items (most of which she didn’t like or need) and felt both relief and remorse after doing so. The acts of theft were not due to revenge or anger. Her kleptomania did not seem related to her marital difficulties. She did display some narcissistic personality traits (such as exaggerated sense of superiority, lack of empathy, lying) that also linked to her need for admiration and attention from various lovers through her numerous affairs. Her lack of other traits (such as indifference, rage, preoccupation with envy), however, did not warrant a narcissistic personality disorder diagnosis. Because the patient’s main concern is her marital difficulties, not kleptomania, marital problems are noted first on the DSM diagnosis below. Axis I: Marital Problem Axis II: Narcissistic personality traits |
PART A
Pyromania - Case Study 10
|
Description A distraught mother brought her six year-old son into a She was especially afraid that he would set their house on fire while she and her 10 year-old daughter slept. Since the boy was four, he had shown an unhealthy fascination with fire. He had set several fires in the past two years, all of which his mother had found and extinguished. She noted that her son was sneaky about setting the fires, making it increasingly difficult for her to monitor. The boy told the doctor that he sets fires because a “man in his head” tells him to – and that he is afraid to disobey the man for fear of physical punishment. The mother does not take this reason seriously as he has given a variety of other reasons in the past, depending on to whom he was speaking. Both mother and son agreed that he started the fires in retaliation against his mom when he was angry with her. The first fire the boy set involved burning holes in plastic bed sheets. When his mother found out, she hit him on the hands and told him about the dangers of fire. The second incident occurred after the mother painted a door frame. Her son tried to burn the door frame with a lighter. He was not hit, but he had his bicycle privileges revoked for one week. The third episode occurred when the mother was asleep. Her son had set the garbage on fire and then beat the fire out with a broom. She awoke to an odd smell and found her son running around the house in a peculiar manner. With the fourth fire, the boy burned a dishtowel and threw it in the garbage. When his mother found out, she sent him to bed. Afterwards she explained how dangerous fires were. The last fire involved a toy in a Styrofoam® box. The boy burned holes in the box where the toy’s feet and arms would be. The mother also found her son attempting to smoke in the bathroom. Once again, she talked about the dangers of fire. She explained that fires get bigger with alcohol and smaller with water. In these discussions, the boy became very excited but promised to stop playing with fire. The mother remarked that her son missed his friends from their old neighbourhood and that he was unhappy in school. She believed that her son had no friends outside of school and that both her children often complained of being bored. Other than the fire-setting behaviour, no other aggressive behaviours were exhibited by the boy. He was occasionally difficult to discipline, but the mother said that was because he ignored her. The boy’s teacher was surprised to hear of the fires. The teacher described the six year-old as lovely, bright, and obedient – a student who worked and played well with others. The 26 year-old mother admitted to becoming violently angry at times, so much so that she was not able to control herself. She even said that she had made her son put his hand in a gas flame to teach him that fire hurts. Later, however, she denied this fact despite the fact that her son confirmed her original story. The boy, except for the burn, was physically healthy. Emotionally, however, he was guarded and distrustful when interviewed. This distrust was due, in part, to fear of his mother’s reaction. Eventually, he shared that he loves to talk about fires. Although he knew that he could get hurt or even killed by fire, he was fascinated by them. When speaking about fires, the boy’s affect was inappropriate. He laughed at the wrong times and/or have blunted emotion when he should have more passionate feelings. He also appeared genuinely frightened of the “man in his head.” |
Diagnosis The setting of fires can be symptomatic of conduct disorder. The six year-old, however, has no other antisocial problems and performed well at school – working well with both peers and his teacher. It is doubtful that he set fires as political statements or for insurance purposes, but evidently he derived much pleasure and excitement from fire and fire-setting. Although documenting such information in a young child is difficult, it can be inferred that there was tension before the boy set the fires. Therefore, the diagnosis is pyromania, an ICD. Because he had no other signs of psychotic behaviour apart from the “man in his head,” and because his reasons for setting the fires varied, an additional diagnosis of a psychotic disorder is not made. His overall diagnosis in Axis I is pyromania. |
 hospital emergency room because she was afraid that she could no longer prevent him from setting fires.
hospital emergency room because she was afraid that she could no longer prevent him from setting fires. PART A
Trichotillomania - Case Study 11
|
Description A young woman sought treatment at a dermatology clinic for her increasing baldness at the crown of her scalp. The clinician did not find any disease relating to a dermatological cause, so the 25 year-old was referred to a psychiatrist. She told the psychiatrist that, since she was a child, she pulled out single hairs from the top of her head after twisting the strand of hair around her finger.
She generally performed the behaviour when alone, tired, bored, or reflecting over a stressful event. After pulling the single hair from her scalp, she would inspect it and run it over her lips. She would continue this behaviour for several minutes at a time. The plucking of the hair did not hurt – in fact, it produced a sense of release. The woman hid her “thinning” hair by wearing it up, but eventually the baldness was too difficult to hide. She sought help when she realized that she may have to wear a wig. The woman also spoke of temper problems, drinking too much, and having unsatisfying relationships. Other than linking her hair-pulling to the childhood absences of her mother, she described no other causal link or health problem. As her treatment sessions progressed, it was learned that the patient had experienced many traumatic events as a child. For example, her father (who was a barber) died from cancer. The patient described herself as clean and orderly, but noted that she smoked a pack of cigarettes per day. She also admitted to experimenting with drugs such as speed and marijuana, but because they made her paranoid, she discontinued their use. |
Diagnosis While stroking and fussing with hair is a common practice for many people, in this case the behaviour of hair pulling increased to the point of alopecia (baldness). The patient was unable to control the desire to pull out her hair, and she experienced a sense of relief from the action. Because no dermatological reason is apparent for the hair loss, these symptoms are sufficient for a trichotillomania diagnosis. Although not in this case, this disorder often begins in childhood and is frequently connected with intellectual disorders (mental retardation). Her DSM diagnosis is Axis I: trichotillomania. |

Lesson Review
Lesson 1 Part A draws to a close. Were you overwhelmed by the amount of material and the number of different ideas presented? Do not dismay! You will likely find future lessons less hectic. If you have managed to understand the main ideas in the lesson notes and are ready to tackle some assignments, you have done well!
|
To summarize: • Panic Disorder: • Obsessive Compulsive Disorder (OCD): • Generalized Anxiety Disorder (GAD): • Phobias: • Eating Disorders: • Impulse Control Disorders: |
Assignment
There is no assignment to complete for this lesson.