Lesson 3: Treatment
| Site: | MoodleHUB.ca 🍁 |
| Course: | Abnormal Psychology 35 RVS |
| Book: | Lesson 3: Treatment |
| Printed by: | Guest user |
| Date: | Thursday, 30 October 2025, 1:14 AM |
Table of contents
- Section/Lesson Objectives
- Introduction
- 1 - Drug Therapy
- 2 - Adlerian Therapy
- 3 -Behavioural Therapy
- 4 - Existential Therapy
- 5 - Gestalt Therapy
- 6 - Person-Centered Therapy
- 7 - Psychoanalysis
- 8 - Rational-Emotive and Cognitive-Behavioural Therapy
- 9 - Other Traditional Therapies
- 10 - Electroconvulsive Therapy
- 11 - Virtual Reality Therapy
- 12 - Humour as a Treatment Method
- 13 - Figure 17.1: Treatment
- 14 - Perception
- 15 - Alberta Statistics
- 16 - What is the economic cost of mental illness?
- 17 - What are the chances of recovering from mental illness?
- 18 - Do children suffer from mental illenss?
- 19 - Is mental illness life threatening?
- Lesson Review
- Assignment
Section/Lesson Objectives
The student will ...
• Understand and describe the three common childhood disorders discussed in the course.
• Discuss the possible causes of Tourette syndrome, autism, and attention deficit hyperactivity disorder.
• Discuss how dissociative disorders develop
• Explain the unique nature of synesthesia
• State the difference between correlation and causation
• Understand the effects of confounding factors in relationships
• Compare and contrast the various treatment methods discussed in the course
• Understand and describe the concept of perceptual blindness
• List the major mental illnesses that Albertans suffer from and state the prevalence of such illnesses in the general population
Introduction
Methods for treating mental illness have improved significantly since the period when bleeding, trephining, and exorcism were used. Current methods are far more humane. Although no one method is best for treating mental illness, some health care practitioners believe most problems can be solved through psychoanalysis. Other practitioners may predominantly use behavioural therapy combined with medication. Although one treatment method may be used successfully with one person, it may not achieve the same results if used with a second person having the same disorder. Mental illnesses are complex, and so, the treatment of mental illness is best approached with an open mind and eclectic view. If one form of treatment is not working, health care practitioners and their patients may need to try another approach. What follows is a partial sampling of the various treatment methods available to individuals.
Drug Therapy
 Just as many physical illnesses can be effectively treated or managed with medication, so can many mental illnesses. Most medication is believed to help restore a state of balance within the brain’s neurotransmitters. Because the brain is a complex organ, physicians, in conjunction with their patients, need to determine the best form and dosage of medication. Some people have allergic reactions to specific drugs, while, for others, the side-effects from the drugs are problematic or worse than the illness itself. In all cases, careful monitoring of the patient drug interaction must occur.
Just as many physical illnesses can be effectively treated or managed with medication, so can many mental illnesses. Most medication is believed to help restore a state of balance within the brain’s neurotransmitters. Because the brain is a complex organ, physicians, in conjunction with their patients, need to determine the best form and dosage of medication. Some people have allergic reactions to specific drugs, while, for others, the side-effects from the drugs are problematic or worse than the illness itself. In all cases, careful monitoring of the patient drug interaction must occur.
Adlerian Therapy
Named for the founder, Alfred Adler, the driving belief behind this therapy is that people are basically “good.” Individuals are in control of their own lives and not victims of “fate.” A therapist gathers the history of the patient, including the patient’s goals and how the patient deals with daily tasks of living. The therapist then uses this information to help set new and more realistic goals for his or her client. In essence, the aims of Adlerian therapy are to confront patients’ belief systems relating to their goals and to encourage and assist them in setting useful goals that increase feelings of competence. Goals range from learning about parenting skills or marital relationship skills to stopping substance abuse or preventing panic attacks. Therapists develop a mutual trust relationship with their clients and, as part of treatment, may assign homework or set up contracts for action.
Behavioural Therapy
Proponents of this form of therapy believe that all behaviours are learned and that people are products of the environment in which they live. The focus is on current behaviour, not past behaviour, which is the result of defective learning. Patients need to model and reinforce functional behaviour with the help of a treatment plan that may include the following:
|
- assertiveness training |
With behavioural therapy, both patient and therapist take active roles in the treatment plan. This type of therapy is commonly used with phobias, sexual dysfunction, stuttering, and depression.

Existential Therapy
Each person has his or her own unique personality. Existential therapists believe people have the freedom to change their personalities if they want. They teach clients that they themselves are responsible for their lives. They focus treatment on the present and future to help patients see that they are responsible for the events in their lives and can work to shape their own futures.
Gestalt Therapy
At the centre of this therapy is the co-ordination of body and mind - specifically the integration of feelings, thinking, and behaviour. Gestalt therapists help clients see how previous experiences shape current behaviours, yet they remind them that people are ultimately responsible for their own actions. Therapists teach patients to avoid problems, to follow through with goals, and to experience things in a positive light. They stress living in the present, not the past or the future. Therapists guide their patients to accept that people must take care of themselves instead of expecting others to do it. Techniques used with this therapy include confrontation, dream analysis, dialogue with polar points of view, and role-playing. This form of therapy is often used in family counselling, childhood behaviour problems, and psychosomatic disorders.

Person-Centered Therapy
Founded by Carl Rogers, this form of therapy gives more responsibility to patients regarding their own  treatment. People are viewed in a positive way with the belief that most individuals can resolve their own problems. Therapists direct their clients through increasing levels of self-awareness and they are encouraged to experience previously denied feelings. Therapists strive to have their clients trust in themselves. With the increasing self-trust they develop, patients begin to direct their own lives. The person-centered therapist guides individuals to uncover their real problems and helps direct them to solutions. They focus on “the here and the now.” With this view, good mental health is a balance between the ideal self and the real self. If there is a large gap between what a person is (real self) and what a person wants to be (ideal self), maladjusted behaviour may result.
treatment. People are viewed in a positive way with the belief that most individuals can resolve their own problems. Therapists direct their clients through increasing levels of self-awareness and they are encouraged to experience previously denied feelings. Therapists strive to have their clients trust in themselves. With the increasing self-trust they develop, patients begin to direct their own lives. The person-centered therapist guides individuals to uncover their real problems and helps direct them to solutions. They focus on “the here and the now.” With this view, good mental health is a balance between the ideal self and the real self. If there is a large gap between what a person is (real self) and what a person wants to be (ideal self), maladjusted behaviour may result.
Psychoanalysis
Psychoanalysts believe that unconscious drives and desires influence behaviour. Therapists also believe that people are guided by both aggressive and sexual impulses. Events during the first six years of life determine personality; unresolved conflicts from this time period may lead to problems in adulthood. Anxiety is a result of the repression of these early conflicts that, combined with unconscious desires, lead to maladaptive behaviour. To develop into mentally healthy individuals, people must successfully progress through the five psychosexual stages listed below.
|
Five Psychosexual Stages - oral stage (birth to one year): sucking |
According to this therapy, if a child does not adequately progress through each stage then personality flaws develop. Therapists will help patients bring their unconscious conflicts into their awareness so they may resolve them. Clients who are self-centered, impulsive, or psychotic generally do not respond well to this type of treatment.

Rational-Emotive and Cognitive-Behavioural Therapy
These action-oriented therapies deal with the cognitive and moral state of individuals. Therapists believe that people have the ability to understand and change their behaviours. Because therapists believe that people are capable of rational thought, they use directed therapy to guide clients in making good decisions. In the view of the therapist, maladaptive behaviour is the result of illogical and irrational thinking. All problems that individuals have are the result of irrational (faulty) belief systems formed in childhood. Therapists work with clients to help them change these irrational belief systems and self-defeating outlooks. In general, the therapist is the teacher and the client is the student.
Other Traditional Therapies
Many other therapies can be used to treat individuals suffering from mental illnesses. Some therapists use reality therapy or transactional analysis while others are experts in neurolinguistic programming and hypnotherapy. Many therapists, however, are eclectic in their treatment methodology. They will use the best techniques from a variety of therapies and may even recommend medication if appropriate. Of the many techniques available to health care practitioners for the treatment of their clients, electroconvulsive therapy many be the most controversial, and virtual therapy may be the most innovative.

Electroconvulsive Therapy
Electroconvulsive therapy (ECT) was developed in the 1930s for use in the treatment of mentally ill people. ECT involves sending an electrical current through the brain at a low voltage. When it was first used, however, the voltage was excessive and almost half of the patients experienced complications (including dislocated joints and broken bones) from being restrained during the violent convulsions that occurred.
Current medical practice of ECT therapy involves anesthetising the patient (making unconscious) then injecting a drug to temporarily paralyze the muscles. In this state, the muscles do not contract during the treatment, thus preventing bone and joint injuries. Electrodes are placed on the scalp and a very small electrical current is passed through the brain. This current produces a seizure that may last from 30 seconds to a minute. About fifteen minutes later, the patient regains consciousness. The patient may experience confusion and have a headache and/or sore muscles for several minutes.
Although psychiatrists do not fully understand why ECT works, they believe the seizures stimulate activity in the synapses between neurons. This activity may restore brain neurotransmitters much like the action of antidepressants. Many health care practitioners prefer to use traditional treatment methods first and suggest ECT only if no improvement in the condition of the patient has resulted. Other psychotherapists actively support banning ECT because they consider it an inhumane and ineffective treatment. One patient, however, credits ECT with improving her life and preventing a potential suicide. Please review her story, summarized from Chatelaine (1998).
|
Läna, a student in university, developed depression part way into her fall semester. The depression became so severe that she considered suicide as an option. She eventually moved back in with her parents and began taking antidepressants prescribed by her doctor. The medication, however, had little effect, and she was hospitalized a few months later. While in the hospital, Läna learned about ECT. Her psychiatrist described the procedure to her and told her that the rate of success was between 60 to 80 percent. She agreed to try ECT and, after about a dozen treatments, began to feel better. In fact, Läna was able to return to school. She earned her degree and now describes herself as happy and energetic. If she were ever to experience severe depression again, Läna commented she would not hesitate to undergo additional ECT sessions. |
Video: How ECT helped a woman with severe depression.
 Although ECT may not be the best treatment for everyone with depression, for severely depressed people who do not respond to antidepressant medications or cognitive therapy, ECT may be the only alternative. Treatment often requires more than six sessions and patients must give consent before beginning this form of therapy.
Although ECT may not be the best treatment for everyone with depression, for severely depressed people who do not respond to antidepressant medications or cognitive therapy, ECT may be the only alternative. Treatment often requires more than six sessions and patients must give consent before beginning this form of therapy.
Virtual Reality Therapy
 Not long ago, virtual reality therapy was used only in science fiction movies. Still in its early phase, this form of therapy appears to be quite promising - not only for those with physical disabilities, but for those with mental disabilities as well. The basis behind this form of treatment is the notion that an effective way to reduce pain, whether emotional or physical, is to distract the person with something else. The “something else” in this case, is a computer-generated “virtual” experience.
Not long ago, virtual reality therapy was used only in science fiction movies. Still in its early phase, this form of therapy appears to be quite promising - not only for those with physical disabilities, but for those with mental disabilities as well. The basis behind this form of treatment is the notion that an effective way to reduce pain, whether emotional or physical, is to distract the person with something else. The “something else” in this case, is a computer-generated “virtual” experience.
All pain, even physical pain, has a powerful psychological component. A pain signal can be interpreted as either more or less painful depending on the mindset of the individual. Virtual therapy is designed to totally immerse patients in another world – to effectively modify their mindsets. In one experiment involving burn victims, patients were distracted with Nintendo games during one treatment and a virtual reality spider phobia program in the second treatment. Even though the burn victims did not have spider phobias (arachnophobia) as the virtual program was designed for, they reported a dramatic decrease in pain while immersed in the two-dimensional virtual world. Other studies confirmed these results and noted that virtual therapy is far more effective than other therapies used with burn victims – even traditional pain control with opioid drugs.
In other trials using virtual technology, burn victims participated in a “ChocolateWorld” scenario. In this program they were able eat a real chocolate bar and “see” the bite marks appear in the virtual chocolate bar! This form of distraction proved quite effective in their pain management. Regarding psychological pain, virtual reality therapy is being used in the treatment of phobias including fear of heights, fear of flying, fear of speaking in public, post traumatic stress disorder, and fear of spiders (Hunter Hoffman, 2004).
In another example, a woman with arachnophobia was willing to try virtual therapy (summarized from  Scientific American, August 2004). The woman had acquired a number of obsessive-compulsive behaviours linked to her phobia. For example, she regularly used pesticides in her vehicle and at home to eradicate any spiders that lived there. She sealed her bedroom windows with duct tape to prevent any spiders from entering her house from the outside. She sealed freshly laundered clothing in plastic bags to prevent “contamination” from spiders. Her condition worsened, so much so that she was hesitant to leave her house. After 20 years of coping with her phobia, she eventually sought help.
Scientific American, August 2004). The woman had acquired a number of obsessive-compulsive behaviours linked to her phobia. For example, she regularly used pesticides in her vehicle and at home to eradicate any spiders that lived there. She sealed her bedroom windows with duct tape to prevent any spiders from entering her house from the outside. She sealed freshly laundered clothing in plastic bags to prevent “contamination” from spiders. Her condition worsened, so much so that she was hesitant to leave her house. After 20 years of coping with her phobia, she eventually sought help.
Similar to other types of treatment, virtual reality therapy may employ systematic desensitization  techniques to help individuals. Regarding our spider-phobic woman, the virtual reality treatment involved gradually introducing her to a virtual spider. Progressively the fear decreased and then she became more comfortable. In the first few sessions of virtual therapy, the woman saw a virtual spider in a virtual kitchen. She approached as close as possible (using a handheld joystick to navigate through the three-dimensional scene) with a goal to come within a metre of the virtual spider. Eventually her goal was to reach for the spider while wearing a special glove that tracked the position of her hand. The spider was then to make a brief noise and flee a few inches away from the “cyberhand”. The women was then instructed to pick up a virtual vase with her cyberhand. When she let go of the vase, the vase remained in midair but an animated spider with wiggling legs came out. The spider then drifted to the floor of the virtual kitchen, accompanied by a brief sound effect from the classic horror movie Psycho. The patient then repeated similar tasks until she reported little anxiety surrounding the virtual spiders.
techniques to help individuals. Regarding our spider-phobic woman, the virtual reality treatment involved gradually introducing her to a virtual spider. Progressively the fear decreased and then she became more comfortable. In the first few sessions of virtual therapy, the woman saw a virtual spider in a virtual kitchen. She approached as close as possible (using a handheld joystick to navigate through the three-dimensional scene) with a goal to come within a metre of the virtual spider. Eventually her goal was to reach for the spider while wearing a special glove that tracked the position of her hand. The spider was then to make a brief noise and flee a few inches away from the “cyberhand”. The women was then instructed to pick up a virtual vase with her cyberhand. When she let go of the vase, the vase remained in midair but an animated spider with wiggling legs came out. The spider then drifted to the floor of the virtual kitchen, accompanied by a brief sound effect from the classic horror movie Psycho. The patient then repeated similar tasks until she reported little anxiety surrounding the virtual spiders.
Our patient then moved on to the next challenge. Her final therapy sessions added tactile feedback to her virtual experience – specifically a toy spider with an electromagnetic position sensor. The toy was suspended in front of the patient, which allowed her to feel the furry object with one hand while touching the virtual spider with her cyberhand. In the end, the patient had a significantly reduced fear of spiders and her obsessive-compulsive behaviours also disappeared. Her specific success was unusual - after treatment she was able to hold a live tarantula for several minutes with little anxiety. It is hoped that the future of virtual therapy will expand to help people cope with more disorders – both physical and psychological.
Video: Virtual Reality Therapy for Panic Disorder, Agoraphobia and Specific Phobias
Humour as a Treatment Method
 You may have heard the old adage that laughter is the best medicine. In reality, laughing does seem to have benefits when used in the treatment of both mental and physical disorders. Laughter is currently being used to help people with a variety of problems from depression and high blood pressure to cancer and anxiety. Laughter has a positive effect on both the human psyche and immune system and, as a result, many health care professionals are incorporating humour into their treatment of mental and emotional disorders.
You may have heard the old adage that laughter is the best medicine. In reality, laughing does seem to have benefits when used in the treatment of both mental and physical disorders. Laughter is currently being used to help people with a variety of problems from depression and high blood pressure to cancer and anxiety. Laughter has a positive effect on both the human psyche and immune system and, as a result, many health care professionals are incorporating humour into their treatment of mental and emotional disorders.
From a cognitive perspective, it appears that when we learn to be open to humour, we increase our ability to see things from more than one perspective. We become more creative. The flexibility that this facilitates helps people to get out of mental “ruts” and improve negative and stereotypical thinking. Laughter also helps people remove sadness and anxiety from their lives. Just as one cannot experience darkness where there is light, a person cannot experience anger where there is genuine laughter (laughter that is not at the expense of another).
Laughing is believed to disrupt the stress response of the autonomic nervous system. Laughter helps with our breathing and boosts tolerance to pain. The immune system increases its production of antibodies and decreases its release of stress hormones. If possible, people should laugh every day!
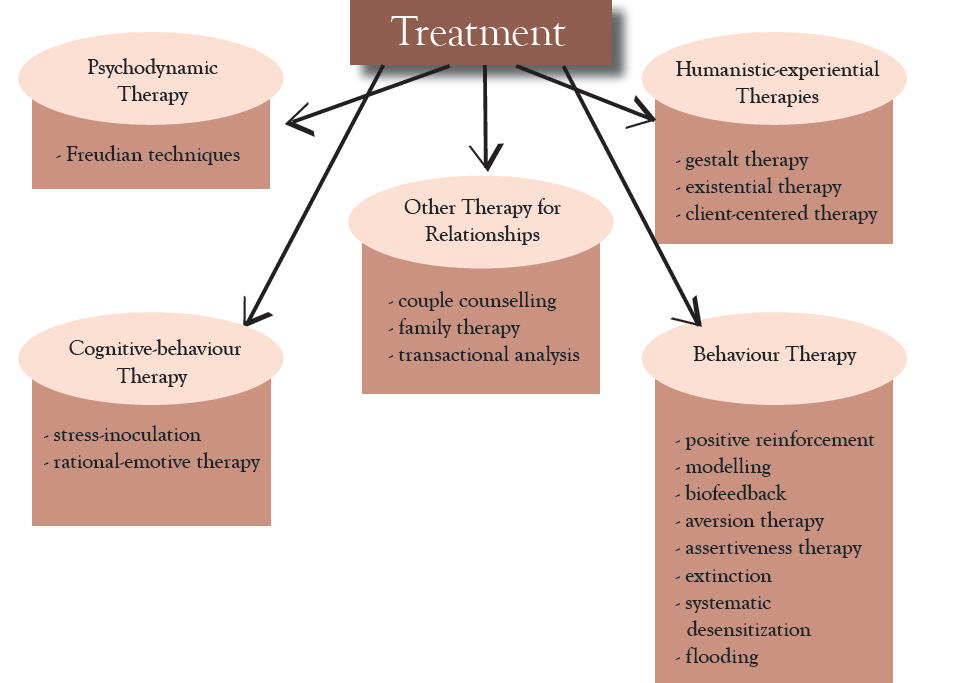
While this course has not described all the available methods used in the treatment of mental illnesses, the following chart provides a broader view of some methods currently available.
Figure 13.1: Treatment
Perception
As stated at the beginning of the course, perception affects behaviour. If we perceive mentally ill people as “bad” or “at fault”, then our opinion of them and our corresponding behaviour toward them reflects this perception. Individuals suffering from mental illnesses are often treated with less dignity than individuals suffering from physical illnesses. The problem is not the mental illness itself, but rather the interpretation we put on it!
People tend to focus their attention on things or events they find interesting or important. It is easy, too, to focus too narrowly or only on the negative aspect of events. When our focus is skewed in this way, we do not get the entire “picture” and our complete understanding of events and situations is compromised. For an example of perceptual blindness, please review the experiment on the next page (summarized from Scientific American, March 2004) that highlights how important our focus is regarding perception and understanding.
Experiment Summary: Perceptual-Blindness
|
Scenario Results Discussion |
Alberta Statistics

|
 The following information, from the Canadian Mental Health Association, highlights statistics regarding mental illness from Canada as a whole, as well as specific statistics regarding the province of Alberta.
The following information, from the Canadian Mental Health Association, highlights statistics regarding mental illness from Canada as a whole, as well as specific statistics regarding the province of Alberta.
| https://www.camh.ca/en/driving-change/the-crisis-is-real/mental-health-statistics |
One in five Canadians will suffer a mental illness at some time in his or her life. If you include addictions to alcohol, drugs and gambling, the number is greater than one in three. You may never develop a mental illness but with those odds, the chances are you will be close to someone who does.
The most common group of mental disorders are anxiety-related and include panic attacks, post traumatic stress, and a whole range of phobias (intense fears). We all experience anxiety in some form, but these “survival” feelings that stimulate our “fight-or-flight” mechanism are perfectly normal. About 12% of the Alberta population will experience anxiety disorders at some time, anxiety that is so intense it immobilizes and affects the ability to enjoy life and deal with day to day experiences and problems.
The second most common category of mental disorders is described as mood disorders and affects about 9% of the Alberta population. Everybody, of course, has “ups and downs” and grieving a loss, for example, is a very natural process. But when these ups and downs (depression and mania) are prolonged over several weeks and are so intense that they take control of our lives, help should be sought.
One of the less prevalent but most misunderstood disorders is schizophrenia, which affects about 1% of the population. Many people think a person with schizophrenia has a “split” or multiple personality. In reality, the person with schizophrenia has a single personality but thoughts, perceptions, and feelings are all mixed up. The person may hear voices or have false beliefs, and in this complex disorganized thinking, it is difficult to know what is real and what is not.
There are dozens of different diagnostic categories in each of the above groupings and many more categories of mental disorder. But almost all of them can be treated, and the recovery rate is higher when treatment is appropriate and given early.
Perhaps as important as treatment is the support of family and friends. Mental disorders still carry a certain stigma or “stain on one’s reputation” caused by misunderstandings. An Ontario survey found that more than 48% of people with a history of mental illness believed that stigma affected their relationships, employment, and housing. This, in turn, affected self-esteem and confidence, causing caution, fear, anger, and depression. The most common public stereotypes are that people with mental illness are untrustworthy, dangerous, weird, and unpredictable.
These stereotypes are in fact myths. People with mental illnesses are no less trustworthy than the general population and only a certain few mental disorders may produce violent episodes and only under certain conditions. In reality, people with mental illnesses are more likely to hurt themselves, or because of their vulnerability, are victims of violence by others. As to being “weird and unpredictable”, a person’s behaviour may be unusual during some episode, but the symptoms are treatable.
In most cases, mental disorders can be viewed as “invisible disorders” seen only from the inside. As for health promotion, we have only begun to understand the nature of mental disorder and how it may be prevented. Some of the answers may be in biology and genetic research. Others will be in nutrition and pharmacology. Income and social status are also important considerations as are education, social support networks, employment and working conditions, physical environments, safety, personal health practices, and coping skills. Still other answers will lie in early childhood nurturing and good parenting.
What is the economic cost of mental illness?
The total economic cost of mental disorders (both medically treated and not) is estimated to be $14.4 billion annually, at a minimum. There is no telling what non-economic costs for pain and suffering should be added to this total. Four of the ten leading causes of disability in developed countries are mental disorders - major depression, bipolar disorder, schizophrenia, and obsessive-compulsive disorder.
What are the chances of recovering from mental illness?
Most people with mental illness recover well and are able to lead fulfilling lives in the community when they receive appropriate ongoing treatment and support. However, only 43% of depressed adults seek care from a health professional.
Do children suffer from mental illness?
Almost 20% of children and youth in Canada, or roughly 1.5 million individuals, suffer from a diagnosable psychiatric disorder. Two-thirds of these suffered from more than one disorder and less than 20% receive therapeutic intervention.
Is mental illness life threatening?
Mental illness itself is not life-threatening. However, more than 90% of people who take their lives (suicide) have a diagnosable mental disorder, commonly a depressive disorder or substance abuse disorder.
The information in Table 18.1 summarizes some of the more common signs of mental illness. The information is adapted from Zuckerman, D., Debenham, K., & Moore, K. (1993) The ADA and People with Mental Illness: A Resource Manual for Employers. According to the Canadian Mental Health Association, sometimes these signs are the result of subtle changes in an individual - such changes often happen gradually over time. Please note that this list is not exhaustive and these signs could be indicative of things other than mental illness.
Table 18.1: Common signs of mental illness
|
Common Signs of Mental Illness
|
| - marked changes in personality - confused thinking - inability to cope with problems and daily activities - strange ideas or delusions - excessive fears, worries, or anxiety - prolonged feelings of irritability or sadness - significant changes in eating or sleeping patterns - thinking or talking about suicide - extreme highs and lows in mood - abuse of alcohol or drugs - excessive anger, hostility - paranoid behaviour - social withdrawal - irrational fears |
In reality, the symptoms in Table 18.1 are not always readily observable in individuals. Sometimes significant changes may be noticed in other areas, however. With respect to school-aged individuals, often changes in work habits, behaviours, performance, and attendance provide good indicators of possible illness. Examples of these changes include the following:
| - consistent late arrivals or frequent absences - low morale - disorganization in completing school work or in study habits - lack of cooperation or a general inability to communicate with others - increased accidents - frequent complaints or evidence of fatigue or unexplained pains - problems concentrating, making decisions, or remembering things - missed deadlines, delays in completing assignments, poor exam grades - making excuses for missed deadlines or poor quality work - decreased interest or involvement in class topics or academics in general |
Please note that individuals who experience problems, such as those previously mentioned, may simply be having a “bad day” or even a “bad week.” They may also be working through difficult times in their lives. A pattern that continues for a long period or is repetitive, however, may indicate an underlying mental health problem or mental illness (Canadian Mental Health Association).
Lesson Review
|
To summarize: Abnormal Psychology 35 is intended to be an introduction to the study of abnormal behaviour. Now that you have completed this course, perhaps you have developed a deeper understanding of what mental illness is and what it is not. You have learned about the differing views of abnormality, the types of psychiatric disorders that can affect people, as well as some of the treatment methods used – both in the past and in the present. You have learned about the importance of the psychologist’s perspective in the analysis of abnormal behaviour. You have learned that anyone anywhere may develop a mental illness at any time. Still, much stigma continues to surround mental illness. With increased knowledge and acceptance, however, people like you are learning that mental illness is not related to weakness of character. Although you may never suffer from a mental illness, you may be close to someone who will. Your understanding and support will help this person cope with their illness with dignity. |
Assignment
Use the Quizzes tool to submit your assignment.
Complete:
1. S4L123Quiz - (Complete this and submit it in the assignment folder).
2. Unit 4 Project Infographic - Treatment Methods
Review the following link on How to Create a Bibliography.
(Submit this in the assignment folder provided at this link: Unit4Project Assignment folder).
If you are creating your assignment in the google drive, save it as a PDF by following these instructions: Converting a google doc to a PDF. Submit the PDF file in the assignment folder.
 Once you have completed these assignments, you just have the final review assignment left to complete. You do not need a password to access it. Please email your teacher if you have any questions.
Once you have completed these assignments, you just have the final review assignment left to complete. You do not need a password to access it. Please email your teacher if you have any questions.
Click on the link below and click "play" for a final course message!